Translate this page into:
Quality of Routine Immunization Services: Trends in some Districts of West Bengal.
Corresponding Author: Dr. Samir Dasgupta, Prof. & Head, Dept. of Community Medicine, Burdwan Medical College, Burdwan
Background:
Routine Immunization remains the cornerstone in child survival initiative throughout the globe. Since launching of Expanded Programme on Immunization (EPI) in 1978 in India during last four decades immunization activities have been evolving, keeping pace with the relentless progress in the field of science of vaccinology. Routine Immunization has been embedded in the reproductive & child health program (RCH)
West Bengal has been one of the better performing states of the country in terms of major RCH indicators like Infant mortality rate, maternal mortality rate, under five mortality rate, coverage of routine immunization etc. Independent assessments done in National Family Health Survey, District Level Household Survey or Coverage Evaluation Survey provide periodic assessment of reach & to some extent quality of services in the country.
Over last few decades, since assessment in NFHS-11 till DLHS-32 (2007-08) there has been consistently an increasing trend of immunization coverage (44% to 76%). However there was wide inter-district variation for this coverage. Moreover, coverage evaluation survey (2009)3 revealed a decline of 10 points from 76% to 65% for the state of West Bengal, for the first time since the independent evaluation started in ‘90s.
GoI declared 2012-13 as the year of Intensification of Routine Immunization, with a fo-cus on improving the immunization coverage in all the districts of the country.4
West Bengal State Immunization Support Cell (WBSISC) is working as a techno mana-gerial support group in the state of west Bengal since 2008. This is a collaborative initia-tive between Department of Community Medicine, Medical College, Kolkata; State Health & Family Welfare department, Govt. of West Bengal & Unicef, West Bengal. Out of nineteen districts in West Bengal, WBSISC had its presence in nine districts, namely Jalpaiguri, Uttar Dinajpur, Malda, Murshidabad, Birbhum, Bardhaman, Purulia, South 24 Pgs & Kolkata till April 2013.
Objective:
General objective:
To assess the trends in quality of Routine Immunization services in the study area.
Specific objectives:
To assess the trend in quality of vaccination in the study area in relation to plan-ning, vaccine-logistic availability, cold chain, injection safety and immunization waste management.
To find out changes in the involvement of different stakeholders in the study area.
Methodology:
Study area: The study was undertaken in all the nine WBSISC project districts of West Bengal, namely, Jalpaiguri, Uttar Dinajpur, Malda, Murshidabad, Birbhum, Bardhaman, Purulia, South 24 Pgs & Kolkata. Routine immunization sessions are regularly conducted in sub centers, out-reach sites, urban health posts and post-partum units of all secondary and ter-tiary care hospitals. Monitoring visits were done at session sites at all levels to collect in-formation.
Study design:
Community based, longitudinal study Study population: The RI sessions sites subcenters, out-reach session, post-partum units of district hospitals, sub divisional hospitals, state general hospitals, medical colleges in both rural & urban areas.
Sampling: Samples of RI sites were selected from a list of planned RI sessions. The facil-ity level assessment was done quarterly of about 12 sessions/quarter. Microplanning unit for RI is the subcenter in rural areas and urban health posts in urban areas. Usually 4-6 sessions are planned per month are held in every routine immunization units like sub cen-ter.
One monitor was scheduled to visit one sessions/day. A rolling workplan was pre-pared by each assessor to cover the district in a quarter.
Techniques:
RI session assessment was done using a standard checklist developed by GoI. The Dis-trict Extenders (DE) engaged by WBSISC were mostly utilized for the assessment. Also the faculty members of the Dept. of Community Medicine, Medical College-Kolkata monitored some of the sessions from time to time. Assessors were trained for using the tool and periodic hand holding support was provided by WBSISC to have a good quality assessment. The assessment tool has gone through multiple revisions over last 5 years, keeping in pace with the evolution and revision of RI progroamme throughout the coun-try. However few basic components have always been part of the assessment tool and we focused on these components for analyzing the trend in quality of routine immunization in the project districts. The tool generates information on site of vaccination, involvement of stakeholders in the session, availability of vaccine and logistics, cold chain, injection safety and waste-management.
Data generated are entered in access based software developed by WBSISC. The data were cross checked and sent to DEs for verification. After cleaning, data were analyzed by SPSS-version 16. Results were presented in tabular and pictorial forms.
Results and discussion:
| Year | Number of Session Visited |
Districts |
|---|---|---|
| Y 2008 | 1357 | Kol BDN PRL JLP MLD DDP UDP MSD |
| Y 2009 | 996 | Kol,BDN,PRL,JLP,MLD,DDP,UDP,MSD,SPG |
| Y 2010 | 1311 | Kol,BDN,PRL,JLP,MLD,DDP,UDP,MSD,SPG,BRB; |
| Y 2011 | 1583 | Kol,BDN,PRL,JLP,MLD,DDP,UDP,MSD,SPG,BRB |
| Y 2012 | 1623 | Kol,BDN,PRL,JLP,MLD,UDP,MSD,SPG,BRB |
| Y 2013(Jan- June) | 605 | PRL,MLD,UDP,MSD,SPG,BRB |
*There had been some changes in project districts from year to year depending on the di-rections of the State Health Dept. Over the years there has been gradual improvement in primary quality indicators on RI. Vaccines should be supplied in vaccine carriers from cold chain point to RI session sites and to maintain cold chain those should be supplied in zipper bags with 4 conditioned ice-packs. In the project districts, more than 80% of sites were having satisfactory cold chain maintenance at session sites. However in 2010 a decline was recorded. Later cold chain handlers training was conducted through-out the state over next two years. Present-ly the indicator shows a steady increase.

- Percentage use of Zipper Bag and $ ice Packs
RI training for Health Workers and Medical Officers gradually covered the majority of the districts by 2011. Writing reconstitution time over the vials of freeze dried vaccines is considered to be an important indicator for quality immunization. It reduces the chance of using reconstituted vaccines beyond stipulated hours of 4 hrs (BCG/Measles) or 2hrs (JE) which may lead to serious AEFI. The indicator is showing a steady increase in last 3 years.
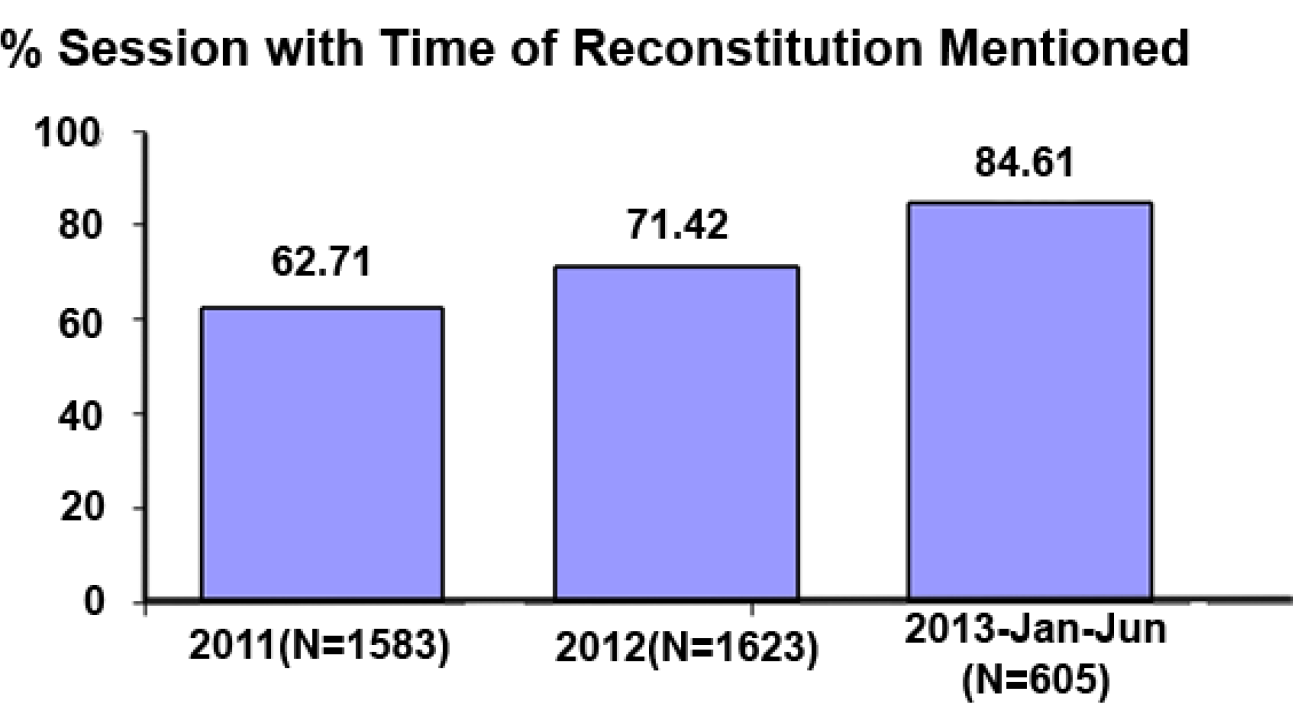
- Percentage of sessions with time of reconstitution mentioned
Auto-disabled syringes have been an important quality input in the RI programme in In-dia. But supply of ADS (especially 0.1ml) is not always regular. At the session sites, use of ADS was assessed and it showed negligible proportion of sessions are now being held without ADS. This practice has been on the steady rise in the RI session sites.

- Uses of Auto disable syringes ( in percentages)
Skill of the vaccinator is key to success in RI. Adherence to recommended site and route for DPT vaccination is an important indicator of knowledge and skill of the vaccinators as improper site and route may cause serious AEFI. Correctness of DPT administration is showing satisfactory improvement.
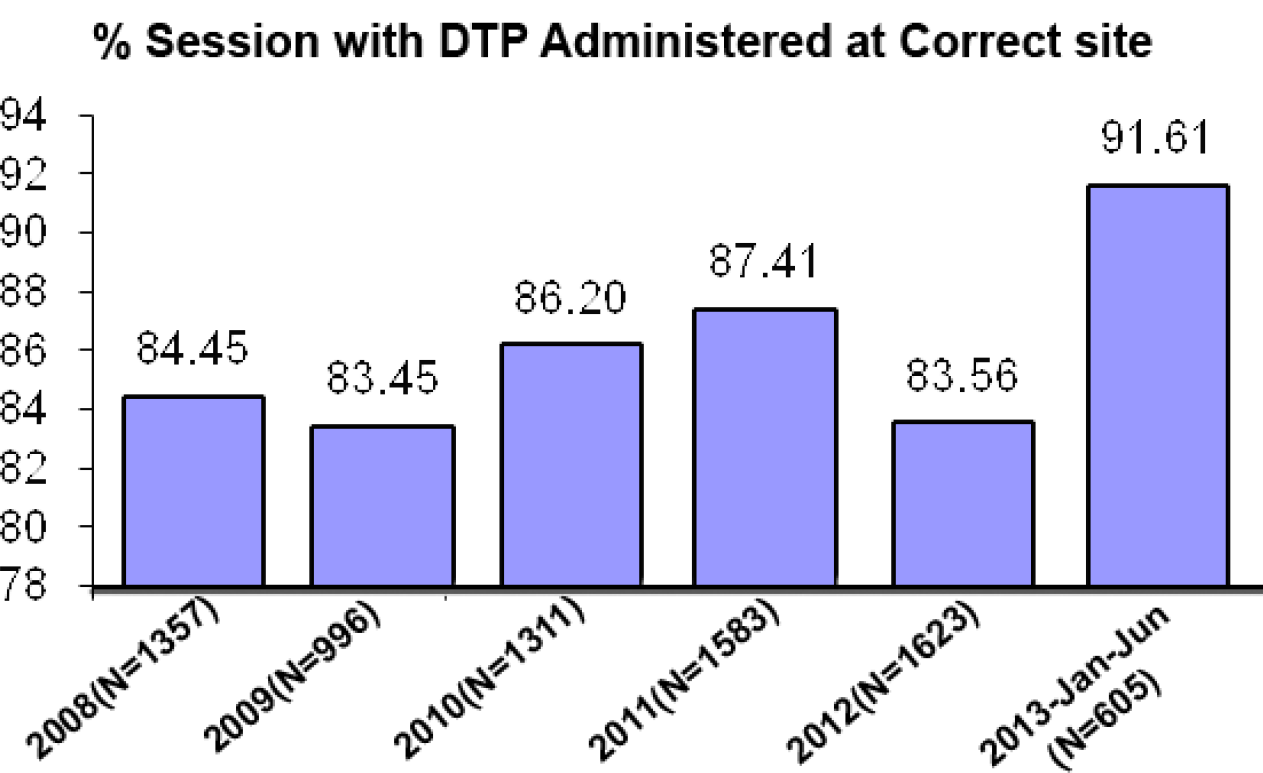
- Percentage of sessions with DPT administered at correct site
Needle touch by ANM undermines the quality. The practice is gradually on the decline. Probably RI training and supportive supervision are responsible to bring down the unsafe practice.

- Percentage of sessions with needle touching by ANM
Use of hubcutter is an important quality indicator linked to immunization waste manage-ment and safe injection practices. In 2008 less than 1/5th of session sites were found to be using hubcutters. After training and ensuring availability, a rising trend in use of hubcut-ter has been observed last 5 years.

- Use of hub cutter (in percentages)
However, there remain several areas of concern where situation is not at all satisfactory. Timely updating and maintenance of counterfoil of MCH/MCP card, communicating the mothers or care-givers the 4-key messages, availability of due list and drop out tracking are some of the issues that still remained deficient. Our monitoring even shows a decline in proportion of sessions with updating counterfoils.
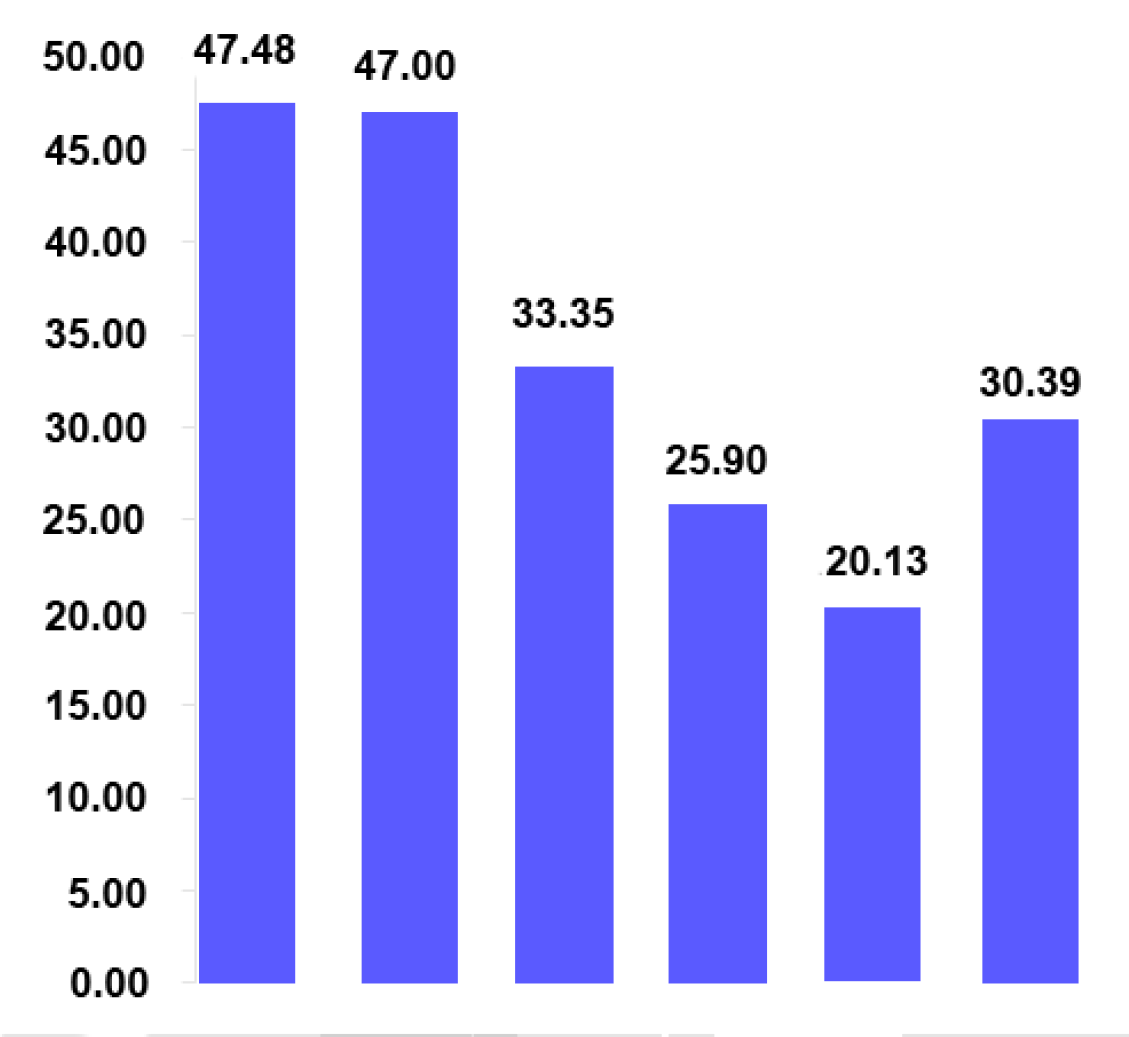
- Percentage of sessions with updating counterfoils(2008-2013)
4-key messages also showed a decline from 43% in 2011 to 27% in 2013
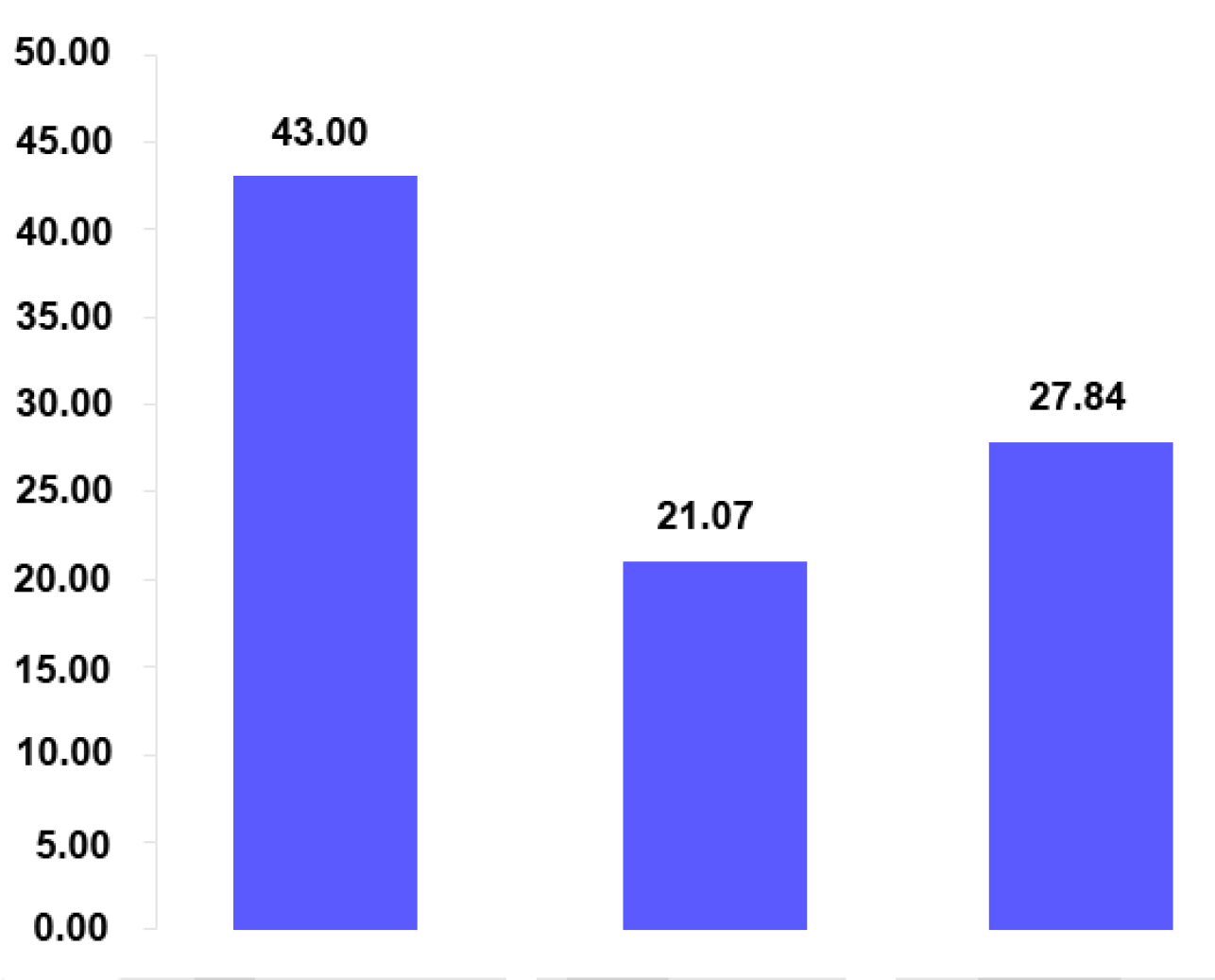
- Percentage of mothers/caregivers communicated 4 key messages (2011-2013)
Conclusion:
Though there was improvement in some quality indicators of RI, there are areas of con-cern. Moreover, analysis of summary values has hidden the range of diversity. There is a wide variation in quality and coverage in the districts. However, with emphasized focus on RI as evident by declaring yr 2012-13 as the year of Intensification of RI, renewed interest has been shown to one of the most cost effective public health programme.
Being on the verge of eradication of wild polio virus from the country we stand in an im-portant juncture to strengthen the RI programme to a robust, sustainable health interven-tion. The scope of RI programme will further widen in coming days with newer eradica-tion targets like measles, introduction of new vaccines and new delivery techniques. Op-erationalization of newer interventions will require a strong service delivery system and the success will depend much on quality assurance. A strong field monitoring system must be in place to identify gaps in the present system and to take remedial measures.
REFERENCES:
- Available from: http://pib.nic.in/newsite/erelease.aspx?relid=79602 (accessed )




