Translate this page into:
Prevalence of Gastroesophageal Reflux Disease And Its Correlates in Adults Residing in an Urban Resettlement Colony of East Delhi
Corresponding Author: Dr. Kartikey Yadav Department of Community Medicine University College of Medical Sciences, New Delhi Email: drkartikeyy@gmail.com
Abstract
Background:
Gastroesophageal Reflux Disease (GERD) is known as a condition caused by abnormal reflux of gastric contents into the esophagus. Most common symptoms include heartburn (a burning sensation in the middle of the chest) and regurgitation (an upward moving sensation of stomach content). GERD Is a distressing medical condition which is under reported. This study was carried out to study the associated riskfactors of GERD.
Objective:
The primary objective of the study was to determine the prevalence of GERD among adults residing in an urban resettlement colony of East Delhi. The secondary objective was to identify the risk factors associated with it.
Methods:
It was a cross sectional descriptive study conducted in Nand Nagri, a resettlement colony in East Delhi from November 2016 to April 2018. The study population comprised of 300 adults (18 and above).For assessment of GERD, Questionnaire for Epidemiology of symptomatic GERD was used.
Results:
The mean age of the study participants was 47.70 years. The prevalence of GERD among study participants was found to be 14.0%. On applying binary logistic regression to find out the predictors of GERD among study participants, female gender, BMI more than or equal to 25, smokers, having comorbid illness, consuming high amount of spices and more than 4 cups of tea or coffee were found to be significant predictors.
Conclusion:
The prevalence of GERD observed in the study was 14.0%. Significant predictors of GERD were female gender, BMI more than or equal to 25, smokers, having comorbid illness, consuming high amount of spices and consuming more than 4 cups of tea or coffee.
Keywords
GERD
Heartburn
Prevalence
Regurgitation

Introduction
Gastroesophageal Reflux Disease (GERD) is known as a condition caused by abnormal reflux of gastric contents into the esophagus. Most common symptoms include heartburn (a burning sensation in the middle of the chest) and regurgitation (an upward moving sensation of stomach content). The Montreal consensus defined GERD as "a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications." Symptoms are "troublesome" if they adversely affect an individual's well-being.
GERD can be diagnosed using a combination of symptoms, 24 hours esophageal pH monitoring, endoscopy and response to anti-secretory medications. Heartburn and regurgitation have been shown to correctly identify GERD with a sensitivity of 89% and specificity of 94%.[1]
The prevalence of GERD varies widely around the world. GERD prevalence was estimated to be 7.1%-13.2% in Asia, 11.5%-19.0% in the Middle East, 12.2-16.2% in Australia, 15.1%-19.1% in Europe, 11.0%-25.3% in South America and 10.7%-20.9% in North America.[2]
Prevalence in India is estimated to be 7.6-25.0%.[3-9] A study done on the employees of a large hospital in New Delhi reported a prevalence of 16.2%.[5]
Compared to Western countries, Asian countries have reported lower prevalence of GERD. Owing to rapid economic growth and Westernization, a large section of population has moved twoards unhealthy litestyle leading to rise in trends of noncommunicable diseases Asia.
Reflux or gastric contents is commonly use to impaired dosure of lower esophageal splincter. [12,11] GERD can cause a gamut of complications that Includes esophageal [esophagitis, Barrett's esophagus and rarely Adenoctardnoma esophngus] as well as eKtrassophageal comphlications such as chropic cough, dysophasia, laryngitis, and asthma-like-symptons.[18]
Heports on the risk factors have been inconsistent among different studies Majority of studies have reported Family Instory, older age, higher socioeconomac status, male gender, incrased BMI, family history, use of Nonsteroidal Anti inflammatoy(NSAIDs) medications, low fruit consumption, smoking and high meat comsumption as Importsnt risk factors.[11,12,13] Whereas few other Studies have stated female gander, fatty diet and shorter dinner-to bed time as significant risk factors.[14,15]
GERD is a distressing medical condition which is under reported. After exterisive literature reviev we found that Very few community based studies on the prevalence of GERD and its Delhi This study amis to address the gap in knowledge in this area.
The primary objective of study was ta assess the prevalence of Gastroesophageal Reflux Disease (GERD) among edult residents of an urban resettlement colony of East Deihi.
Materials and Methods:
This cross sectional study was done in Nand Nagri, a resettlement colory located in East Delhi. it has a population of 65,000. Nand Nagri is divded into 5 blacks (A, B, C, D and E) which have been furthers (divided into 21 sub-blacks having around 10,000 household in total. The study was conducted between November 2016 to April 2018. With an expected prevalence of GERD taking 95% 7.6% canfiden intervel and 3% absolute precision the sample size was calculated as 298, using Epi info 7.2.0 This was rounded of to 300 to select number of participants from each sub-block. Aduits sged 18 years and above resding in Nand Nagri for more than 6 months were included Pregenet women, subjects Who had undergone GIT sufgery or taking NSAIDS for 3 monnths were excluded.
Sampling Pracedure- Sampling was done in 2 stages. in fast stage, sub-block was selected randoxniy from each bolack-A4, B5, C2, E1 in the second stage 60 households were selected from each sub black using clrcular systermatic random sampling Except C2, all sub-blocks have 500 households. In crder to get 60 households from each block, sampling interval was cbtined by dividing the number of households by 50. For blocks A4, B5, D3 and E1 the interval was 8th households whereas for C2 the Interval was 11th households. After selecting the household, all eligible individuals residing in the household were listed and interviewed One participant was selected randomly and interviewed by the investgatro. If the household was found locked even after 3 visits subsequent household in the ascending order was included in the study without disturbing the original allocation.
Study ΤoοΙs- A pretested structured, interviewer administratored questionnaire was used to get the desired information.
PART 1: Information about socio-demographic, anthropainetric profile and other relevant medical history. This stuctored questionnire about sociodemographic detail included questions abouts the age, education and occupation of the study participants, socioeonomic status and type of family details about history of any medical liness and medication histary were also rocorded.
PART 2: For assessment of Gastroesophageal Relux Disease, Questionnaire for Epidemiology of symptomatic GERO was used. It is a questionnaire based diagnostic tool developed by Sharma et al[7] used in Delhi and ladakh.[4] This is based on symptom of heartburn and regurgitation. The final score ranged form 0 to 18. The presence of GEAD was defined as a score ≥4.[8]
Case definition- Heartburn was defined as a burning sensation behind the sternum in the antcrior chest. Regurgitation was defined as a bitter or sour tasting fluid spontaneously coming in to the mouth. Symptom score was calculated using the sever ity and frequency of the individual symptoms [Table 1]. The final score for each symptom i.e. heartburn and regurgitaion was obtained by multiping the score for snverity and frequency. The total score was obtalned by adding the final scouces of individual symptoms Thus the final score rariged from 0 to 18. The presence of GERD.
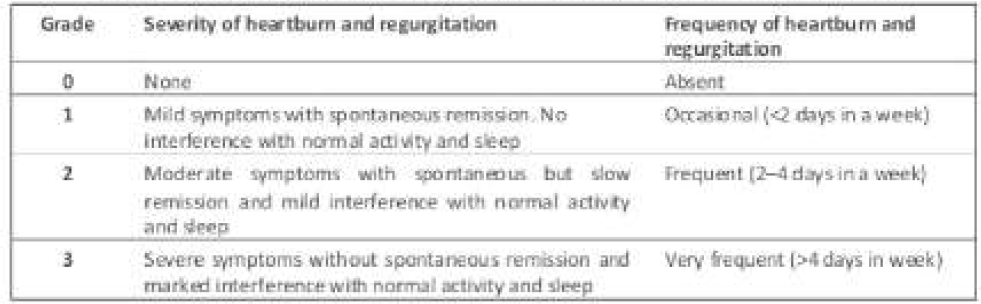
was defined as a scoce ≥ 4, GERD was further classified as mild, moderate and severe based on the final symptom score range of 4-8, 9-13 and 14-18, respectively.[4]
Date management and statistical anahysis- The data was entered into Microsoft Excel and cleaned. The cleaned data was analyzed using SPSS 20.0. The statistical analysis comprised of caiculating means and proportions. Chi-square (Fischer's exact if required) was used to test the statistcal association of GERD with vanous factors. The level of singiticanca was token as pc 0.05. To find out the predictors of GERD, binary iogistic regression was applicd taking GERD as the dependentvariabie. Forward stepwised ratio (LR) was applied to find out the significant predictors. The criseria for cntcring and removing the variables into the regrssion model was p<0.05.
Results:
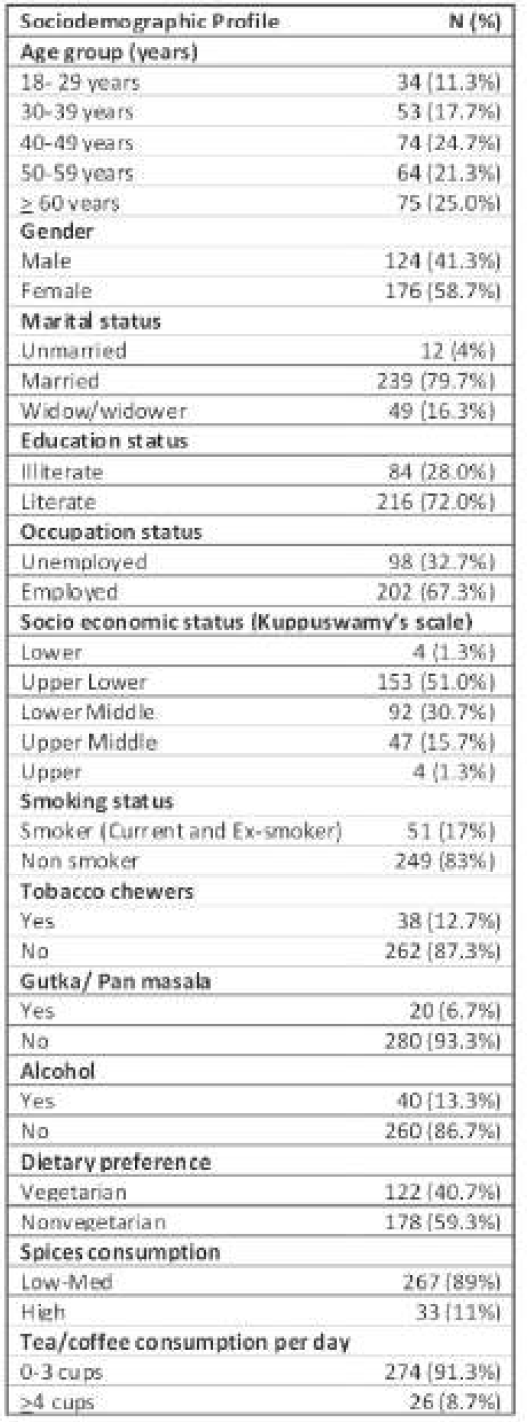
Baseline chartacteristics of study participants are shawn in Table 2. The mean age of study participants was 47.70 years± 14.34(SD) with maximum age beirg 19 years and maximum age being 86 years.
Of 300 study parting. 42[14%] had symptom score ≥ 4, the out-off for defining it GERD. Ninety one (30,3%) study particpants compiained of heartburn occurred on a daily basis (>4 days in a week) in 13 (4.3%) individuals, on a weekty basis (2-4 days in a week) in 25 (8.3%) individuals, and occasionally (<2 days in a week) in 25 (17.7%) Forty-free (15%) individuals complained of regurgitation occurred on a daily basis (>4 days in a week) in 11 (3.6%) individuals on a wockly basis 12-4 days in a weekl in 14 (4.7%). and occasionally (<2 days in a week) in 20 (6.7%) individuals. Based on symptom score of heartbum and regurgitation, GERD is dassified into mild [4-8], moderate [9-13] and severe (14.18). Twenty seven (64.3%) has mid GERD, 7(16.7%) had modenrate GERD and 8(19.0%) has severe GERD, Table 3 shows distrbution of frecuency and severity of GERD symptoms.
| Symptom | Frequency | |||
|---|---|---|---|---|
| Heartburn (n=91) | Occasional (<2 times a week) |
Frequent (2-4 times a week) |
Very Frequent (>4 times a week) |
|
| No GERD(< 4) | 44 | 3 | 2 | |
| GERD (≥4) | Mild (4-8) | 0 | 2 | 1 |
| Moderate (9-13) | 6 | 11 | 2 | |
| Severe (14-18) | 3 | 9 | 8 | |
| Regu rgitation( n=45) | ||||
| No GERD( <4) | 7 | 0 | 0 | |
| GERD (≥4) | Mild (4-8) | 0 | 2 | 1 |
| Moderate (9-13) | 11 | 9 | 3 | |
| Severe (14-18) | 2 | 3 | 7 | |
| Predictor Variable | B | S.E. | Adjusted Odds Ratio (95% C.I.) |
p- value |
|---|---|---|---|---|
| Gender | ||||
| Male | 1* | 0.046 | ||
| Female | 0.821 | 0.411 | 2.272(1.015-5.085) | |
| Body Mass lndex(BMI) | ||||
| BMI<25 kg/m2 | 1* | 0.001 | ||
| BMI ≥25 kg/m2 | 1.245 | 0.387 | 3.473(1.625-7.421) | |
| Smoking status | ||||
| Non-Smoker | 1* | 0.010 | ||
| Smoker ( current + Ex-Smoker) | 1.229 | 0.476 | 3.419(1.346-8.690) | |
| Spices consumption | ||||
| Low to Med | 1* | 0.014 | ||
| High | 1.250 | 0.509 | 3.489(1.286-9.462) | |
| Co-Morbidity Illness | ||||
| No | 1* | <0.001 | ||
| Yes | 1.432 | 0.392 | 4.186(1.940-9.033) | |
| Tea/ coffee consumption | ||||
| 0-3 cups | 1* | 0.044 | ||
| >3 cups | 1.134 | 0.564 | 3.109(1.029-9.400) | |
*Reference category
Discussion:
Gastroesophageal relux disease is charctcrlzcd by refiux of gastric contents into esophagus 11 can also causdyphagia (difflculty in swallowing) and odynophagla (painful deglintion). It may also by associated with extraesophageal symptoms like tooth decay and gingivitis it is the most common cause of non-cardiac of prosperecus people hence, in developing countries like India, GERD was not considered as a signilcant health problem until now. However, the prevalence of GERD has been increasing in india gradually, which may be attributed to the rapidly developing economy and consequent changes which are taking place in diet and lifestyle. In the present study add the prevalence of GERD was found to be 14% as estimated using Questionnaire for epidemiology of GERD. [4,5] The prevalence of GERD ranges from 7.6% to 25.0% in different studies conducted in India.[3-6, 8, 9] The prevalence in our study was considerably higher as compared to studies done in other Asian countries like China, Japan, Iran, Bangladesh, Nepal.[20,21] This could be attributed to various sociocultural and dietary habits in different Asian countries. GERD is more common in western world with prevalence as high as 52%[22]. Several studies done in USA, Nigeria, Greece have reported prevalence of GERD higher than the present study. [22,23] Higher prevalence in Caucasians as compared to Asians might be due to increased dietary fat consumption, higher BMI, lower prevalence of Helicobacter pylori infection (which is negatively associated with GERD)[24] and genetic factors.
Female gender was found to be a significant predictor of GERD in our study. Several studies done in India [4,6,8] as well as outside India [21,25,27] have reported higher prevalence of GERD among females. Studies have shown that prevalence of non- erosive reflux disease was more in females whereas males were more likely to be associated with erosive esophagitis.[28, 29]ln the present study, mean BMI of the participants was 23.23±2.39 kg/m2.The prevalence of GERD among those who had BMI more than or equal to 25 kg/m2 was 24.7% as compared to 10%, among the individuals who had BMI less than 25 kg/m2 which was found to be statistically significant. Several studies have reported significant positive relationship between BMI and GERD[5-7,8,10,26,30] whereas few studies have not observed significant relationship.[3,4] El serag et al.[31] did a cross sectional study and reported that obese people had increased risk of GERD, as increased abdominal obesity leads to increased mechanical pressure on the stomach, thus promoting reflux of gastric contents into esophagus. This lead to increased exposure of esophagus to gastric acid. Murray et al.[32] reported that obesity was significantly associated with severity of GERD and obese individuals were likely to experience heartburn and regurgitation almost three times as compared to individuals who had normal weight. Cigarette smoking is known to adversely affect the defense mechanisms against reflux of gastric contents into the esophagus. Smoking leads to transient reduction in lower esophageal sphincter pressure, reducing salivary output and increased acid clearance time.[33] In present study prevalence of GERD in smokers was significantly higher than non- smokers. Several studies have reported similar findings[5,9,22] whereas few studies haven't observed relationship between smoking and GERD.[4, 6-8] Parietal cells in stomach are responsible for secretion of gastric acid. Spices stimulate these cells and lead to increased acid secretion. In the present study, prevalence of GERD was more in Individuals consuming high amount of spices. Some other studies have also reported similar findings.[34] Tea is one of the most frequently consumed beverage in India. Both tea and coffee contain caffeine. Caffeine stimulates parietal cells and lead to increase gastric acid secretion.[35] In the present study addthe prevalence of GERD in individuals consuming more than four cups of tea was 30.8% as compared to 12.4% in individuals having 0-3 cups to tea/coffee, this association was found to be statistically significant. Several studies have observed significant association between tea/coffee consumption and presence of GERD symptoms.[36,37] Certain drugs trigger or worsen the GERD by either reducing the tone of lower esophageal sphincter, causing increased gastric acid secretion or delayed gastric emptying. Consumption of these drugs can predispose an individual to develop GERD. In present study, the prevalence of GERD in individuals not consuming any medications (11.4%) was less as compared to 23.8% in individuals taking medicines. This association was found to be statistically significant on univariate analysis, but after adjusting with other variables in Binary logistic regression, it was not found to be significant. Wong et al.[38] have observed the association of calcium channel antagonist/nitrates and the presence of GERD whereas others did not find similar association.[5,37] The prevalence of GERD among individuals having selected co-morbid Illness (Hypertension, Diabetes Mellitus, Bronchial Asthma and Heart disease) was 26.5% as compared to 7.9% in other group. This association was statistically significant. On univariate analysis, presence of hypertension and diabetes mellitus was observed statistically significant. Several studies have observed significant association between GERD and hypertension. [5, 6, 26] It may be due to antihypertensive medication as they reduce lower esophageal sphincter tone. There was no association of Asthma with GERD in our study, but a study conducted by Sharma et al.[5] found significant association between Asthma and GERD. In our study, diabetes was significantly associated with GERD whereas Sharma et al.[5] had observed no such association.
The strengths of our study were that it was a community based study to find out the prevalence of GERD among adults. To the best of our knowledge, this is the first study to be conducted in community setting in Delhi. Investigator has recorded the symptoms of GERD and evaluated heartburn and regurgitation using a validated symptom score questionnaire.
The limitations of our study were that It was conducted in Nand nagri, a resettlement colony in East Delhi. Due to manpower and time constraints participants from other areas of Delhi could not be Included. Hence the results of the current study cannot be extrapolated to the whole of Delhi. Heartburn and regurgitation are cardinal symptoms of GERD, but atypical or extraesophageal symptoms of GERD were not taken into consideration. Hence, the study may be providing an under estimate of the disease burden.The study design was a cross sectional one. So the temporal relationship could not be established between the observed risk factors and GERD.
Conclusion
The prevalence of GERD among study participants was found to be 14.0%. As per the severity of GERD, 64.3% had mild GERD, 16.7% had moderate GERD and 19.0% had severe GERD. On applying binary logistic regression (usingforward LR selection model) to find out the predictors of GERD among study participants, female gender, BMI more than or equal to 25, smokers, having comorbid illness, consuming high amount of spices and more than 4 cups of tea or coffee were found to be significant predictors.
Acknowledgement
We would like to thank Dr. Vineet Ahuja for giving us the permission to use the questionnaire.
Conflict of interest:
None
How to cite this article: Yadav K, Saini NK, Patra S, Avasthi R. Prevalence of Gastroesophageal reflux disease And Its correlates in adults residing in an urban resettlement colony of East Delhi. J Comprehensive Health 2019;7(2): 44-49.
Reference:
- Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut. 2018;67(3):430-40.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology and symptom profile of gastroesophageal reflux in the Indian population: report of the Indian Society of Gastroenterology Task Force. Indian J Gastroenterol. 2011;30(3):118-27.
- [CrossRef] [PubMed] [Google Scholar]
- Population based study to assess prevalence and risk factors of gastroesophageal reflux disease in a high altitude area. Indian J Gastroenterol. 2011;30(3):135-43.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, severity, and risk factors of symptomatic gastroesophageal reflux disease among employees of a large hospital in northern India. Indian J Gastroenterol. 2011;30(3):128-34.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, perceptions and profile of gastroesophageal reflux disease in a rural population of North Bihar. Indian J Gastroenterol. 2014;5(2):214-8.
- [Google Scholar]
- Prevalence of gastro-esophageal reflux disease and its risk factors in a community-based population in southern India. BMC Gastroenterol. 2016;16:36.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and the risk factors of gastro-esophageal reflux disease in medical students. Medical Journal Armed Forces India. 2018;74(3):250-4.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of gastro esophageal reflux disease among medical students in Chennai, South India. Indian Journal of Forensic and Community Medicine. 2017;4(3):199-203.
- [Google Scholar]
- The epidemiology of gastroesophageal reflux disease: a survey on the prevalence and the associated factors in a random sample of the general population in the Northern part of Iran. Int J Mol Epidemiol Genet. 2013;4(3):175-82.
- [Google Scholar]
- The gastro-esophageal reflux disease questionnaire using Indonesian language: a language validation survey. Med J Indones. 2011;20(2):125-30.
- [CrossRef] [Google Scholar]
- Extraesophageal manifestations of gastroesophageal reflux disease: cough, asthma, laryngitis, chest pain. Swiss Med Wkly. 2012;142
- [CrossRef] [PubMed] [Google Scholar]
- The Montreal definition and classification of gastroesophageal reflux disease: a global evidence- based consensus. Am J Gastroenterol. 2006;101(8):1900-20.
- [CrossRef] [PubMed] [Google Scholar]
- American Gastroenterological Association Institute technical review on the management of gastroesophageal reflux disease. Gastroenterology. 2008;135(4):1392-413.
- [CrossRef] [PubMed] [Google Scholar]
- Systematic review: geographical and ethnic differences in gastro-oesophageal reflux disease. Aliment Pharmacol Then. 2004;20(7):705-17.
- [CrossRef] [PubMed] [Google Scholar]
- The prevalence of gastroesophageal reflux disease among hospital employees. Dis Esophagus. 2014;27(5):403-8.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for gastroesophageal reflux disease, reflux esophagitis and non-erosive reflux disease among Chinese patients undergoing upper gastrointestinal endoscopic examination. World J Gastroenterol. 2007;13(45):6009-15.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of 24-h esophageal pH monitoring on the diagnosis of gastroesophageal reflux disease: defining the gold standard. J Gastroenterol Hepatol. 2005;20(1):30-7.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of five maintenance therapies for reflux esophagitis. N Engl J Med. 1995;333(17):1106-10.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological study of symptomatic gastroesophageal reflux disease in China: Beijing and Shanghai. Chin J Dig Dis. 2000;1:2-8.
- [CrossRef] [Google Scholar]
- Gastro- oesophageal reflux disorders among Nepalese residing in Southeast Asia. Med J Malaysia. 2013;68(3):234-8.
- [Google Scholar]
- Gastroesophageal reflux disease symptoms in the Greek general population: prevalence and risk factors. Clin Exp Gastroenterol. 2016;9:143-9.
- [CrossRef] [PubMed] [Google Scholar]
- Gastroesophageal Reflux Disease: A Population Based Study. Gastroenterology Res. 2009;2(3):152-6.
- [CrossRef] [Google Scholar]
- Long-term prospective follow-up of endoscopic oesophagitis in southern Chinese-prevalence and spectrum of the disease. Aliment Pharmacol Ther. 2002;16(12):2037-42.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of heartburn and gastroesophageal reflux disease in the urban Brazilian population. Arq Gastroenterol. 2005;42(2):122-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and Correlates of Gastroesophageal Reflux Disease in Southern Iran: Pars Cohort Study. Middle East J Dig Dis. 2017;9(3):129-38.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and risk factors for gastro-esophageal reflux disease in the North-Eastern part of Bangladesh. Bangladesh Medical Research Council Bulletin. 2013;38(3):108-13.
- [CrossRef] [PubMed] [Google Scholar]
- Differences in clinical characteristics between patients with endoscopy-negative reflux disease and erosive esophagitis in Japan. Am J Gastroenterol. 2005;100(4):754-8.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative analysis between psychological and endoscopic profiles in patients with gastroesophageal reflux disease: a prospective study based on screening endoscopy. J Gastroenterol Hepatol. 2006;21(5):798-804.
- [CrossRef] [PubMed] [Google Scholar]
- The Prevalence and Risk Factors of GERD among Indonesian Medical Doctors. Makara Journal of Health Research. 2016;20(2):35-40.
- [CrossRef] [Google Scholar]
- Obesity increases oesophageal acid exposure. Gut. 2007;56(6):749-55.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between body mass and gastro- oesophageal reflux symptoms: The Bristol Helicobacter Project. International Journal of Epidemiology. 2003;32(4):645-50.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of cigarette smoking on gastropharyngeal and gastroesophageal reflux. Ann Oto I Rhinol Laryngol. 2001;110(2):190-3.
- [CrossRef] [PubMed] [Google Scholar]
- Gastroesophageal reflux disease among population of Arar City, Northern Saudi Arabia. Electron Physician. 2017;9(10):5499-505.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of coffee and caffeine on gastrin and acid secretion in man. Dtsch Med Wochenschr. 1976;101(12):455-7.
- [Google Scholar]
- An epidemiological study of gastroesophageal reflux disease and related risk factors in urban population of mashhad, iran. Iran Red Crescent Med J. 2014;16(12):el5832.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology and risk factors of uninvestigated dyspepsia, irritable bowel syndrome, and gastroesophageal reflux disease among students of Damascus University, Syria. J Epidemiol Glob Health. 2016;6(4):285-93.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, clinical spectrum and health care utilization of gastro-oesophageal reflux disease in a Chinese population: a population-based study. Alimentary Pharmacology and Therapeutics. 2003;18(6):595-604.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors associated with symptoms of gastroesophageal reflux. Am J Med. 1999;106(6):642-9.
- [CrossRef] [PubMed] [Google Scholar]




