
Translate this page into:
Cardiovascular Disease Risks Related to Consumption of Ready-To-Eat Food Products between Young Adults of Kolkata, West Bengal, India

-
Received: ,
Accepted: ,
How to cite this article: Roy Choudhury S, Das P, Koner S, Ghosh J, Singh K. Cardiovascular Disease Risks Related to Consumption of Ready-To-Eat Food Products between Young Adults of Kolkata, West Bengal, India. J Compr Health. 2024;12:60-5. doi: 10.25259/JCH_11_2023
Abstract
Background:
Cardiovascular diseases (CVDs) are the leading cause of mortality worldwide. In 2010, ischemic heart disease and strokes together claimed the lives of an estimated 13 million people globally, making about 25% of all deaths (compared to barely 1 in 5 deaths two decades previously). Over the past few decades, there has been a notable global growth in the consumption of ultra-processed foods. The term “ready-to-eat” or “ultra-processed foods” (UPF) refers to “formulations of ingredients, mostly for industrial use only, derived from a series of industrial processes”. UPF contributes significantly and steadily to the world’s food supply.The amount of industrially processed foods in the world’s food supply has expanded simultaneously with the incidence of obesity and non-communicable illnesses in many nations. They often have lower fiber and vitamin density, higher levels of added sugar, salt, saturated fat, and energy density, as well as a higher concentration of many of these nutrient supplements and characteristics that are particularly linked to cardio metabolic health.
Objectives:
Objective of the study is to understand the cardiovascular disease risks related to consumption of ready-to-Eat (RTE) food products among young adults in Kolkata, West Bengal, India.
Material and Methods:
This cross-sectional study was conducted among young adults, both male and female, between the ages of 20 and 30 who were living in Kolkata. The study duration was from April to July 2021. The same size was N = 150. The KAP (Knowledge, Attitude, and Practice) method was used in this study. The pretested, standardized questionnaires were made on the Google form, and the link was sent through the social media platform to the randomly selected people. Data was put in a Microsoft Excel worksheet (Microsoft, Redwoods, WA, USA) and checked for accuracy. The association between two attributes was calculated by Pearson’s chi-squared test using Statistical Package for the Social Sciences software (SPSS), version 20.0 (SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered statistically significant.
Results:
In this cross-sectional study, 44.18% of males and 38% of females are overweight, whereas 39.71% of the population is ready to eat food on a regular basis. The consumption varies from one to three times a day. This regular consumption of ultra-processed and ready-to-eat (RTE) food, which is significantly associated with high BMI and overweight, can be a cause of cardiovascular, coronary heart, and cerebrovascular disease, respectively.
Conclusion:
To reduce the negative effects of ready-to-eat foods on obesity and cardiovascular health, it is essential to prioritize whole, unprocessed foods in the diet.
Keywords
Obesity
Ready-to-eat food
Cardiovascular disease
Obesity

INTRODUCTION WITH OBJECTIVES
Globally, cardiovascular diseases (CVDs) constitute the primary cause of death. In 2010, an estimated 13 million individuals worldwide died from ischemic heart disease and strokes combined, accounting for 25% of all fatalities worldwide (compared to just one in five deaths two decades prior).1 This growth conceals a significant difference in global patterns and epidemiology for various geographical areas. Developed nations like Western Europe, North America, Australia, and New Zealand are often seen as being at the fourth (very advanced) stage of the health burden phenomenon, which is also known as the “epidemiological transition”2 From the perspective of CVD, the epidemiological shift implies that infection-related illnesses such as rheumatic heart disease and disorders affecting the heart muscle caused by nutritional deficiencies would decline in industrialized countries. On the other hand, due to changing lifestyles and longer life expectancies, developing economies have a much higher age-adjusted prevalence of noncommunicable illnesses, including CVD.3 The Fourth Universal Definition of Myocardial Infarction was modified to include out-of-hospital abrupt cardiac death when defining myocardial infarction.4 The Rose Angina Questionnaire was used to determine stable angina. The World Health Organisation’s definition of stroke was used for estimation, and it was divided into three subcategories: (1) Intracerebral hemorrhage; (2) subarachnoid hemorrhage; and (3) ischemic stroke.1
The consumption of ultra-processed foods (UPFs) has significantly increased during the last several decades throughout the world. According to the NOVA categorization, UPFs that are also known as ready-to-eat (RTE) foods are “formulations of ingredients, mostly for industrial use only, derived from a series of industrial processes.”5 Breakfast cereals, salty snacks, frankfurters, pre-packaged frozen foods, soft and/or sweetened drinks, distilled alcoholic beverages, and supplements are some examples of UPF. UPF is a significant and expanding component of the global food supply. According to recent studies, these items make up a sizable portion of the average American, Canadian, or British consumer’s daily diet, or roughly 50–60% of the energy content.6-8 In many countries, the prevalence of obesity and non-communicable diseases has increased at the same time that the number of industrially processed items in the global food supply has increased9 raising the possibility of a connection. They frequently contain total fat, saturated fat, added sugar, salt, and energy density, as well as less fiber and vitamin density (12–25); many of these nutritious supplements and attributes that are specifically relevant to cardiometabolic health. It is a technical era in the modern world. With each advancement in daily duties, life has already become more straightforward, to the point where less work is required from people.10 Human labor is being replaced by technology in a number of areas including entertainment and the supply of essential human needs.11 Up until a certain time, technology was more of a convenience than a need. Products that have been converted from their natural state to a new state through chemical, mechanical or physical processing in processing businesses or at home are referred to as RTE items.12,13 These goods include food that has been homogenized, dried, dehydrated, condensed, frozen, pasteurized, fried, and dried again. The domestic and international food processing industries play a significant role in connecting farmers with their ultimate customers biological and physiological variables.14 The objective of the present study is to understand the impact of RTE food among young adults in Kolkata, West Bengal, India.
MATERIAL AND METHODS
This cross-sectional study was conducted among young adults, both male and female, between the ages of 20 and 30 who were living in Kolkata. The study duration was from April to July 2021. The same size was n = 150. The knowledge, attitude, and practice (KAP) method was used in this study (26). The pretested, standardized questionnaires were made on the Google form, and the link was sent through the social media platform to the randomly selected people. For those who did not have access to the internet, a telephone conversation was arranged for them to collect the data. The questionnaires used in the study were closed-ended questions, and they were divided into two parts. The first part consisted of some questions regarding personal information, and the second part consisted of questions about KAP regarding RTE food products. Questions about knowledge regarding RTE food products were asked to know how much information they had about them. Questions about attitude toward RTE food products were asked to get knowledge about their mentality and perceptions toward RTE food products. Questions about practice were asked to get information about the application of knowledge regarding RTE food products in their daily lives.
Statistical analysis
Data was put in a Microsoft Excel worksheet (Microsoft, Redwoods, WA, USA) and checked for accuracy. The association between two attributes was calculated by Pearson’s Chi-squared test using Statistical Package for the Social Sciences software (SPSS), version 20.0 (SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered statistically significant.
RESULTS AND DISCUSSION
As shown in Figure 1, just 1.56% of males are generally underweight compared to 54.68% who are of normal weight, 34.38% who are overweight, and 9.38% who are obese. Only 8% of women overall are obese, compared to 30% who are overweight, 60.67% who are normal weight, and 1.33% who are underweight. Compared to 59.29% of individuals who are of normal weight, 30.09% of people who are overweight, and 9.74% of people who are obese, only 0.88% of consumers who are members of nuclear families are overweight [Figure 2]. Only 2% of the respondents in the joint family are underweight compared to 64.86% who are of normal weight, 29.73% who are overweight, and 2.71% who are obese. Only 1.47% of the 150 consumers who consume RTE snacks are underweight, 58.82% are of normal weight, 32.36% are overweight, and 7.35% are obese [Table 1]. No one is underweight; 78.57% of consumers who do not consume RTE snacks are of normal weight; 7.14% are overweight; and 14.29% are obese. Only 0.75% of customers who purchase RTE items out of convenience are underweight while 62.69% are normal, 27.61% are overweight, and 8.95% are obese [Table 1]. A total of 1.75% of RTE customers are underweight compared to 52.64% who are normal weight, 33.33% who are overweight, and 12.28% who are obese [Figure 2]. A total of 0% of people who buy RTE items on average every two to three days are underweight, 63.85% are normal weight, 30.12% are overweight, and 6.03% are obese. One in every 16 RTE customer is underweight whereas 83.33% are of normal weight and only 16.67% are fat. Moreover, 1.33% of those who occasionally buy RTE goods are underweight compared to 60.67% who are of normal weight, 30% who are overweight, and 8% who are obese. The frequency of purchasing RTE food products is significantly associated with body mass index (BMI) according to Pearson’s Chi-square test (χ2 =17.761, P = 0.038). Those who do use RTE products for convenience range in weight from 6.25% underweight to 50% overweight, with no one being obese [Figure 3]. The BMI of the customers and their use of RTE items for convenience have a significant association (χ2 = 7.913, P = 0.04), according to Pearson’s Chi-square test. Consumers who were influenced by pricing while purchasing the product,as shown in Table 1, are 1.41% underweight, 54.92% normal weight, 36.62% overweight, and 7.05% obese. Consumers who are not impacted by price include those who are underweight (2.23%), normal weight (64.44%), overweight (24.44%), and obese (8.89%). No one is underweight; 67.64% of consumers who indicated they might have an opinion on checking the price while buying RTE are 67.64% normal weight, 23.53% are overweight, and 8.83% are obese. Furthermore, it shows that among those who are aware that trans fats raise the risk of CVDs, 1.10% of participants are underweight, 59.34% are of normal weight, 31.87% are overweight, and 7.69% are obese. About 8.33% of participants who are aware that trans fats do not pose a serious threat to health are underweight, 25% are at a healthy weight, 41.67% are overweight, and 25% are obese. Among all the participants who are unaware of trans fats, 0% are underweight, 72.34% are considered normal, 23.40% are overweight, and 4.26% are considered obese. The Pearson Chi-square test shows a significant relationship between BMI and consumer knowledge of trans fats (χ2 = 15.174, P = 0.019). Only 1.61% of customers who were influenced by packaging before purchasing RTE were 1.61% underweight, whereas the other 54.84% were normal, 33.87% were overweight, and 9.68% were obese. The average consumer who occasionally gets influenced by packaging is 66.67% normal, 27.16% overweight, and 6.17% obese. About 14.29% of shoppers who never get influenced by packaging are underweight compared to 42.86% who are of normal weight, 28.57% who are overweight, and 14.28% who are obese. The Pearson Chi-square test reveals a significant association between consumers’ BMI and how frequently they check prices (χ2 =12.552, P = 0.044) [Figure 4]. Figure 4 predisposes the correlation matrix of different parameters of Ready to eat (RTE) consumption pattern among the targeted population.
| Parameters | BMI | |||||
|---|---|---|---|---|---|---|
| Under weight n(%) | Normal n(%) | Over weight n(%) | Obesity n(%) | Total (n) | Chi-square (P) | |
| Do you consume RTE snacks? | ||||||
| Yes | 2 (1.47) | 80 (58.82) | 44 (32.36) | 10 (7.35) | 136 (100) | 4.474 (0.215) |
| No | 0 (0) | 11 (78.57) | 1 (7.14) | 2 (14.29) | 14 (100) | |
| Do you consume RTE for convenience? | ||||||
| Yes | 1 (0.75) | 84 (62.69) | 37 (27.61) | 12 (8.95) | 134 (100) | 7.913, (0.04) |
| No | 1 (6.25) | 7 (43.75) | 8 (50) | 8 (50) | 16 (100) | |
| How often do the consumers check the price while buying RTE? | ||||||
| Yes | 1 (1.41) | 39 (54.92) | 26 (36.62) | 5 (7.05) | 71 (100) | 3.616 (0.73) |
| No | 1 (2.23) | 29 (64.44) | 11 (24.44) | 4 (8.89) | 45 (100) | |
| May be | 0 (0) | 23 (67.64) | 8 (23.53) | 3 (8.83) | 34 (100) | |
| Do consumers have any knowledge about trans-fat? | ||||||
| They increase the risks of CVD | 1 (1.10) | 54 (59.34) | 29 (31.87) | 7 (7.69) | 91 (100) | 15.174 (0.019) |
| They are not that bad for your health. | 1 (8.33) | 3 (25) | 5 (41.67) | 3 (25) | 12 (100) | |
| Do not know | 0 (0) | 34 (72.34) | 11 (23.40) | 2 (4.26) | 47 (100) | |
| Does packaging influence you to buy RTE products? | ||||||
| Always | 1 (1.61) | 34 (54.84) | 21 (33.87) | 6 (9.68) | 62 (100) | 12.552 (0.044) |
| Sometimes. | 0 (0) | 54 (66.67) | 22 (27.16) | 5 (6.17) | 81 (100) | |
| Never | 1 (14.29) | 3 (42.86) | 2 (28.57) | 1 (14.28) | 7 (100) | |
RTE: Ready-to-eat, BMI: Body mass index, CVD: Cardiovascular disease

- Distribution of body mass index (BMI) according to the consumer genders n = 150.
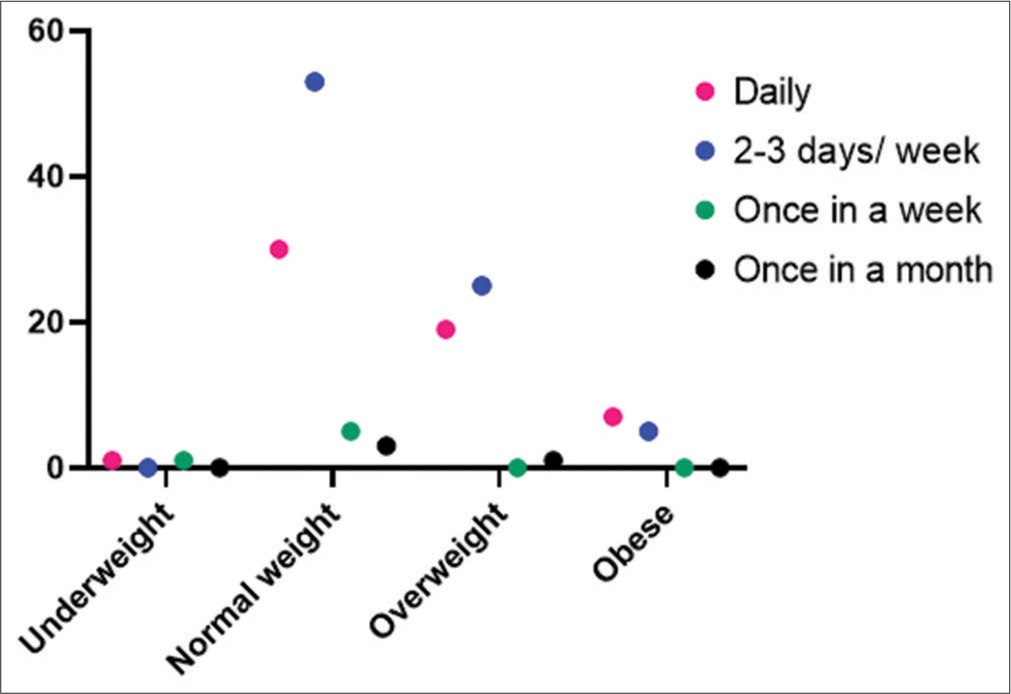
- Distribution of body mass index (BMI) with respect to frequency of purchase of ready-to-eat food products n = 150.
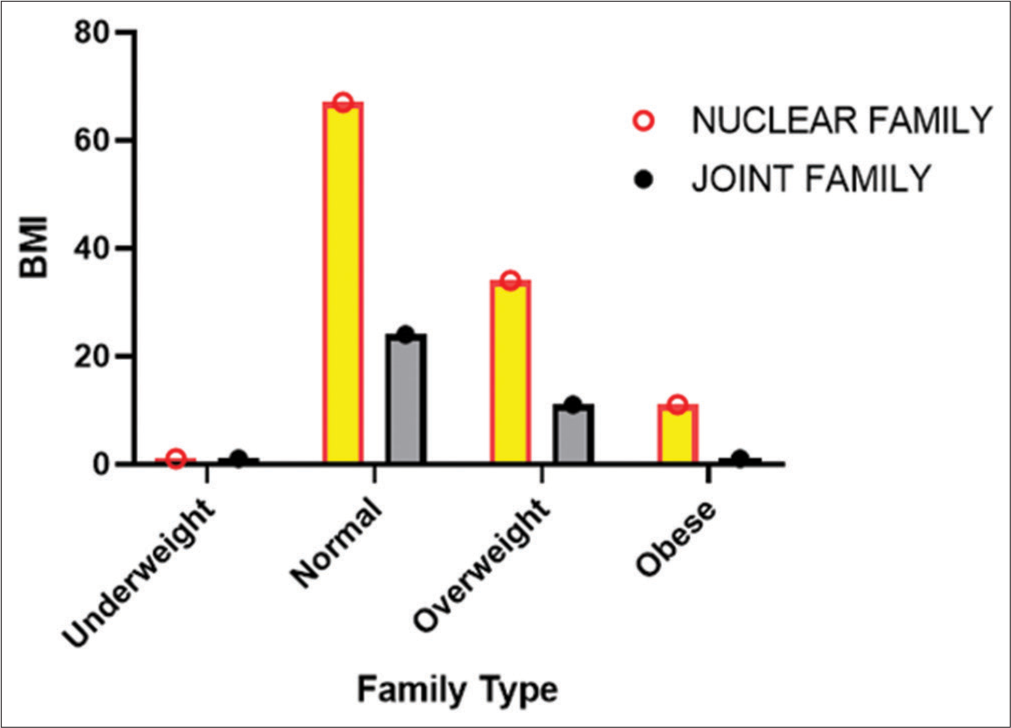
- Distribution of body mass index (BMI) with respect to family type of the consumers.

- The association matrix between the target variables is shown in Figure 4. When there is a noteworthy substantial association between ready to eat (RTE) intake and employment position. Light blue shade implies poor correlation between the variables, whereas red denotes high correlation. On the right side of the picture is a representation of the color indicator. BMI: Body mass index.
DISCUSSION
In this cross-sectional study, 44.18% of males and 38% of females are overweight whereas 39.71% of the population is RTE food on a regular basis.15 The consumption varies from one to three times a day. This regular consumption of ultra-processed and RTE food, which is significantly associated with high BMI and overweight, can be a cause of cardiovascular, coronary heart, and cerebrovascular disease, respectively.16,17 First of all, compared to unprocessed or homemade foods, UPFs typically have a lower nutritional quality since they tend to be higher in sodium, calories, fat, and sugar while being lower in fiber.18,19 They also have a stronger glycemic response. High levels of evidence support the risk factors for cardiometabolic health associated with several of these nutritional components — high sodium, saturated fat, added sugars, and inadequate dietary fiber.19 A diet rich in fruits and vegetables and low in saturated fats is said to be able to cut the occurrence of new cardiac events by as much as 73%.20,21 But still, for Indian college students, the circumstances are comparatively distinct. Before turning eighteen, professionals estimate that in India, parents’ norms have a significant influence on students. And cultural norms, which govern and supervise how they exercise and what they consume. More than that age, their education ends, and they reach adulthood and are able to make their lifestyle selections. This makes people between the ages of 18 and 25 more susceptible. Changing ages and being presented with a variety of options make people more likely to lead unhealthy lifestyles.21-25
CONCLUSION
The prevalence of obesity and CVD is on the rise and RTE foods, which are frequently high in refined carbohydrates, unhealthy fats, and excessive sodium, play a key role in this trend. These accessible solutions frequently contain excessive amounts of empty calories while being deficient in vital elements. Consuming them encourages weight gain and interferes with metabolic health. In addition, consuming too much salt and trans fats can increase cholesterol and blood pressure, which increases the risk of CVD. Regular consumption of these processed foods displaces better-for-food, whole-food alternatives, aggravating the issue. To reduce the negative effects of RTE foods on obesity and cardiovascular health, it is essential to prioritize whole, unprocessed foods in the diet.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Cardiovascular Diseases (CVDs) Fact Sheet. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) [Last accessed on 2018 Jun 01]
- [Google Scholar]
- Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation. 2016;133:187-225.
- [CrossRef] [PubMed] [Google Scholar]
- Decline in Cardiovascular Mortality. Circ Res. 2017;120:366-80.
- [CrossRef] [PubMed] [Google Scholar]
- Sudden Death after Myocardial Infarction. JAMA. 2008;300:2022-9.
- [CrossRef] [PubMed] [Google Scholar]
- Ultra-Processed Foods: What They are and How to Identify Them. Public Health Nutr. 2019;22:936-41.
- [CrossRef] [PubMed] [Google Scholar]
- Ultra-processed Foods and Added Sugars in the US Diet: Evidence from a Nationally Representative Cross-sectional Study. BMJ Open. 2016;6:e009892.
- [CrossRef] [PubMed] [Google Scholar]
- Consumption of Ultra-Processed Foods Predicts Diet Quality in Canada. Appetite. 2017;108:512-20.
- [CrossRef] [PubMed] [Google Scholar]
- Ultra-processed Food consumption and Chronic non-communicable Diseases-related Dietary Nutrient Profile in the UK (2008-2014) Nutrients. 2018;10:587.
- [CrossRef] [PubMed] [Google Scholar]
- Ultra-processed Food and Adverse Health Outcomes. BMJ. 2019;365:l2289.
- [CrossRef] [PubMed] [Google Scholar]
- The Second Machine Age: Work, Progress, and Prosperity in a Time of Brilliant Technologies United States: WW Norton and Company; 2014.
- [Google Scholar]
- Food Processing Technology: Principles and Practice United Kingdom: Woodhead publishing; 2022.
- [Google Scholar]
- A New Service-quality Model to Enhance Customer Retention in the Hong Kong Fast-food Restaurant Industry (Doctoral Dissertation, Faculty of Business and Law, The University of Newcastle, Australia)
- [Google Scholar]
- Assessment of Consumption Patterns of Soft Drinks and Its Impact on Nutritional Status among Young Adults of Kolkata. Int J Sci Res Arch. 2023;8:1050-8.
- [CrossRef] [Google Scholar]
- Ultra-Processed Food Intake and Risk of Cardiovascular Disease: Prospective Cohort Study (NutriNet-Santé) BMJ. 2019;365:l1451.
- [CrossRef] [PubMed] [Google Scholar]
- Ultra-processed Food Consumption is Associated with Increased Risk of All-cause and Cardiovascular Mortality in the Moli-sani Study. Am J Clin Nutr. 2021;113:446-55.
- [CrossRef] [PubMed] [Google Scholar]
- Characterizing Ultra-processed Foods by Energy Density, Nutrient Density, and Cost. Front Nutr. 2019;6:70.
- [CrossRef] [PubMed] [Google Scholar]
- Diet and Cardiovascular Disease. 2013. Geneva, Switzerland: World Heart Federation; Available from: http://www.world-heart-federation.org [Last accessed on 2013 Sep 23]
- [Google Scholar]
- A Review on Understanding the Risk Factors for Coronary Heart Disease in Indian College Students. Int J Noncommun Dis. 2023;8:117-28.
- [CrossRef] [Google Scholar]
- Prevalence of Risk Factors for Obesity, Hypertension, Coronary Artery Disease and Diabetes among Under-graduate Medical College Students of Tamil Nadu. Int J Community Med Public Health. 2017;4:3250-5.
- [CrossRef] [Google Scholar]
- Magnitude of Behavioural Risk Factors for Cardiovascular Diseases among College Going Young Adults (18-25 Years) in Mysuru, Karnataka, India. Int J Community Med Public Health. 2017;4:65-72.
- [CrossRef] [Google Scholar]
- Prevalence of Tobacco and Associated Risk Factors among University Law Students in Indore City. Indian J Dent Res. 2019;30:10-4.
- [Google Scholar]
- Prevalence of Constipation and Its Relationship with Dietary Habits Among College Going Girls in the Age Group of 18-25 Years of Kolkata, West Bengal, India. Acta Sci Gastrointest Disord. 2023;6:3-13.
- [CrossRef] [Google Scholar]
- Media Influence on Dietary Practices among Young Adults of Kolkata. Acta Sci Nutr Health. 2022;6:9-15.
- [CrossRef] [Google Scholar]




