Translate this page into:
Community Based Study on Reproductive Tract Infection in a District of West Bengal - An Appraisal
Address for correspondence: The Editor/ Managing Editor, Journal of Comprehensive Health Dept of Community medicine NRS Medical College, 138, AJC Bose Road, Kolkata-700014
Corresponding Author: Prof. (Dr.) Anima Haldar, HOD Community Medicine, NRS Medical College; 138,A. J. C Bose Road, Kolkata - 700014
Abstract
Background:
Reproductive tract infections and sexually transmitted diseases represent a major public health problem in developing countries. As reported from different community based studies conducted in India, the range of self reported morbidity vary from 39- 84%. Majority of the women bear the problems silently without seeking advice and treatment. Objectives: to estimate the prevalence of RTIs morbidity among married women and identify different socio-environmental factors associated with it.
Materials & Methods:
A Community Based Cross - Sectional study was carried out in Howrah district of West Bengal during May 2009 to August 2009 to reveal the prevalence of Reproductive Tract Infection and its Social correlates. The respondents were 2000 currently married women (15-49yrs) selected by stratified multistage random sampling. House to house visit and data collection was done by faculty members of Community Medicine of different Medical colleges of W.B. using predesigned & pretested schedule.
Result:
The prevalence of RTI was 9.9% and was higher in 24-29 yrs age group. RTI was indirectly proportional to literacy status. Prevalence of RTI was significantly higher among those who did not use sanitary napkin or clean sundried domestic cloths. The occurrence of RTI was lower among those who used to practice barrier method of Contraception whereas it was higher among Cu-T users. Majority of symptomatic complained about vaginal discharge (44.7%).
Conclusion:
To prevent RTI morbidities, use of clean sundried domestic cloths, barrier method of contraception and awareness about small family norm are to be recommended through intervention in future.
Keywords
RTI
Social correlates
Contraceptive

INTRODUCTION
Reproductive tract infections and sexually transmitted diseases represent a major public health problem in developing countries.1 The annual incidence of RTI/STI in India is estimated at 5%, approximately 40 million of new infections take place every year2. The consequences of RTIs are numerous and potentially devastating which include post abortal and puerperal sepsis, ectopic pregnancy, foetal and perinatal death, cervical cancer, infertility, chronic physical pain, emotional distress and social rejection of women.3 As reported from different community based studies conducted in India, the range of self reported morbidity vary from 39- 84%.(4,5) In developing countries both the incidence/prevalence of RTIs/STIs are very high, they rank second as the cause of healthy life lost among women of reproductive age group after maternal morbidity and mortality6. Majority of the women bear the problems silently without seeking advice and treatment7-8.
So, with these above perspectives, the present community based cross sectional observational study was conducted to estimate the prevalence of RTIs morbidity among married women and identify different socio-environmental factors associated with RTI.
MATERIAL & METHODS
A community based cross-sectional observational study was undertaken in May 2009 to August 2009 by stratified multistage random sampling. The study population were currently married women of Howrah district of West Bengal. The sample size was calculated by considering prevalence of RTI as 50% and permissible level of error as 5% and was calculated as 1600. Out of total 14 blocks of Howrah district, 3 blocks had been selected randomly. From each rural block, 2 sub-centres and from each sub-centre areas 2 villages had been selected randomly. Total 4 wards were selected randomly from two municipality areas. So a total of 16 units (4 villages from each block and 2 wards from each municipality) had been chosen for study purpose. From each village/ ward 125 couples were selected to obtain a total sample size of 2000. The data were collected using a predesigned, pretested questionnaire interviewing the female partner of all couples in a house to house survey using standard technique. The study variables were age, age at marriage, literacy level, age at first conception, parity, birth interval, current use of contraceptives, ever use of contraception, RTI morbidities.RTI morbidities includes pain lower abdomen, vaginal discharge, pruritus vulve, low back pain, genital ulcer, inguinal bubo based on syndromic approach as recommended by Govt of India. All women with reproductive tract infection related morbidity were asked to consult nearby BPHC/ Sub-divisional or District hospital.
Data analysis was done with the help of Microsoft Excel and Epi-Info (3.5.4) software.
RESULTS
The present study revealed that only 9.85% reported symptoms suggestive of reproductive tract infection. Table-I indicated the relationship between socio-environmental co-relates and RTI. Vaginal discharge was the commonest symptom found (Fig-I). Prevalence of RTI was maximum (11.39%) in 24-29 years age group and minimum (6.51%) in age group 18-23 years. The difference was statistically significant. The prevalence of RTI was higher (46.18%) among illiterate & just literate group, least (6.6%) in graduate and above group educated group. The difference was statistically significant. Majority of women belonged to poor social class (53.5%) and very poor (BPL) comprised 33.6% of surveyed women; RTI prevalence was higher (12.0%) among BPL group and lowest (6.89%) among high social class group.
| Variables | Total surveyed / No of participants |
No of symptomatic RTI cases No Percentage |
Statistical Test | |
|---|---|---|---|---|
| Age group (yrs.) | ||||
| < 18 | 21 | 2 | 9.5 | X2 = 8.43, df = 3, p = 0.03 |
| 18 - 23 | 491 | 32 | 6.5 | |
| 24 - 29 | 632 | 72 | 11.4 | |
| 30 -35 | 573 | 59 | 10.3 | |
| ≥ 36 | 283 | 32 | 11.3 | |
| Education | ||||
| Illiterate | 538 | 86 | 15.9 | X2 = 137.2, df = 4, p = 0.0001 |
| Just literate | 129 | 39 | 30.2 | |
| Primary | 426 | 47 | 11.0 | |
| Secondary | 802 | 78 | 9.7 | |
| ≥ Graduate | 105 | 7 | 6.7 | |
| Type of family | ||||
| Nuclear | 1400 | 132 | 9.4 | X2 = 0.97, df = 2, p = 0.616 |
| Joint | 560 | 61 | 10.9 | |
| Other | 40 | 4 | 10.0 | |
| Social Class (Rs.) | ||||
| Upper High (> 10000) | 4 | 0 | 0.0 | X2 = 5.962, df = 4, p = 0.202 |
| High (5000-9999) | 29 | 2 | 6.9 | |
| Upper middle (3000-4999) | 33 | 3 | 9.1 | |
| Lower (1500-2999) | 191 | 15 | 7.8 | |
| Poor(500-1499) | 1070 | 96 | 8.9 | |
| BPL (< 500) | 673 | 81 | 12.0 | |
Regarding contraceptive practices, reproductive tract infections was lower (6.1%) among those who used to practice barrier method of contraception whereas it was 16.4% and 12.2% among Cu-T users and those who had undergone permanent sterilisation respectively (Table - II).
| Variables | Total surveyed / No of participants |
No of symptomatic RTI cases No Percentage |
Statistical Test |
|
|---|---|---|---|---|
| Age at marriage (yrs.) | ||||
| < 18 | 1102 | 114 | 10.3 | X2 = 0.97, df = 2, p = 0.614 |
| 18 - 23 | 842 | 79 | 9.4 | |
| 24 - 29 | 48 | 4 | 8.3 | |
| ≥ 30 | 8 | 0 | 0 | |
| No. of Children | ||||
| No issue | 676 | 50 | 7.4 | X2 = 14.75, df = 4, p = 0.0052 |
| 1 | 836 | 79 | 9.4 | |
| 2 | 359 | 48 | 13.4 | |
| 3 | 96 | 14 | 14.6 | |
| ≥ 4 | 33 | 6 | 18.2 | |
| Contraceptive use | ||||
| None | 779 | 70 | 8.9 | X2 = 9.693, df = 5 p = 0.084 |
| Condom | 148 | 9 | 6.1 | |
| OCP | 507 | 44 | 8.8 | |
| Cu-T | 61 | 10 | 16.4 | |
| Ligation | 368 | 45 | 12.2 | |
| Vasectomy | 2 | 0 | 0.0 | |
| Other | 135 | 19 | 14.1 | |
| Use of Sanitary napkin / clean sundried domestic cloths | ||||
| Yes | 462 | 21 | 4.5 | X2 = 19.03, df = 1, p = 0.000013 |
| No | 1538 | 176 | 11.4 | |
| Total | 2000 | 197 | 9.9 | |
Fig-I indicated that majority (45%) suffered from vaginal discharge followed by others (25.8%), pain abdomen (15.6%), low back pain (15.2%) and least suffered from dysuria (4.9%).
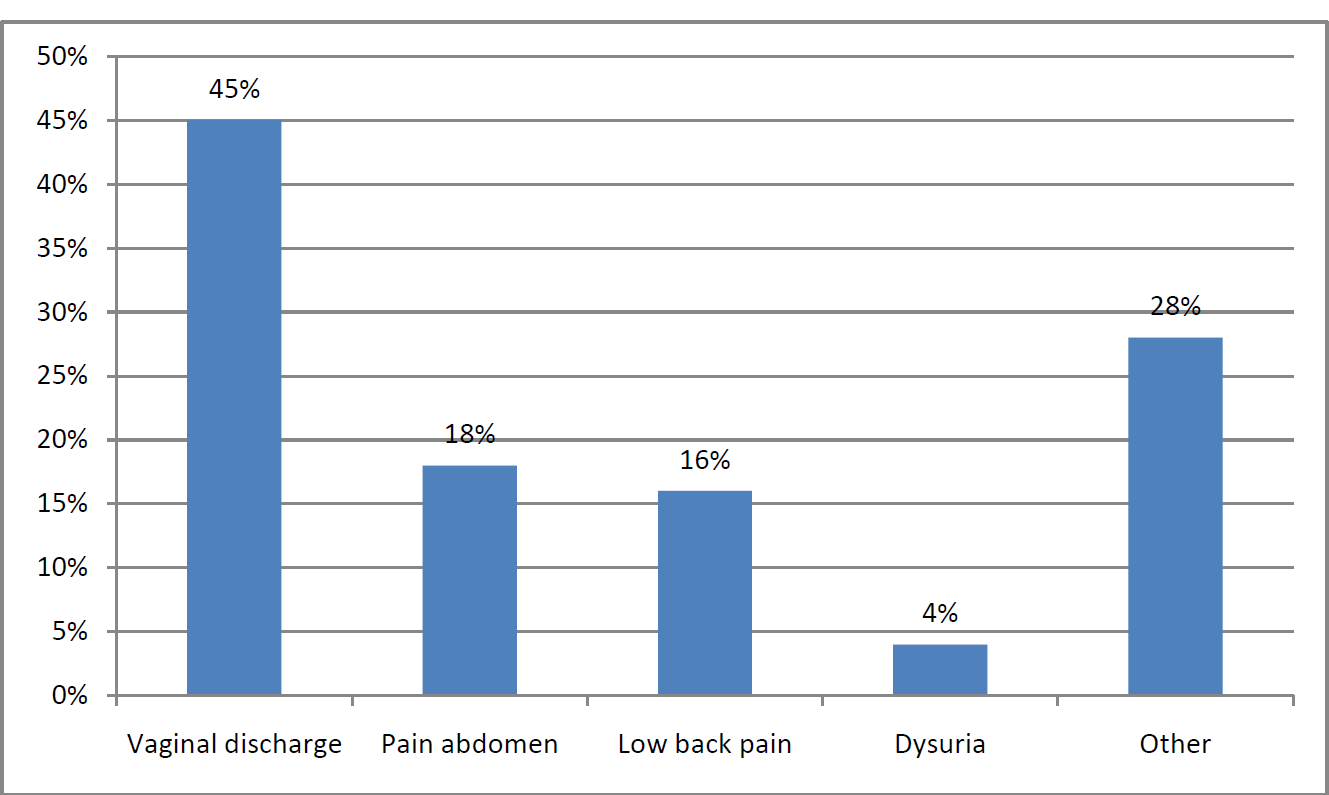
- Symptoms wise distribution of RTI cases
Regarding health seeking behaviour majority (57.8%) prefer to attend private practitioner followed by Govt hospital (45.8%) and 12.8% of the respondents also favoured quacks (Table- III).
| Fertility | No. | Percentage |
|---|---|---|
| Pvt. Practitioner | 1155 | 57.8 |
| Govt. Hospital | 916 | 45.8 |
| Nursing Home | 78 | 3.9 |
| Quacks | 256 | 12.8 |
| Ayurvedic | 53 | 3.2 |
| Homeopathy | 100 | 5.0 |
| Health worker | 101 | 5.1 |
| Others | 6 | 0.3 |
Discussion
The present study revealed low prevalence of Reproductive tract infections (9.85%) in married women of age 15-49 years, probably due to accessibility of health care services. But earlier community based studies reported higher prevalence of RTIs4,9-11. The prevalence of RTIs/ STDs was found to be 49% in a rural area of district of Agra10 and 70% in rural area of Haryana11.Prevalence of RTI observed by studies done in slum and rural areas of Chandigarh12,13 was 21.6%,17,7% respectively. Prevalence of RTI was reported 29% in earlier study8 also 35.3% and 51.9% RTI prevalence reported from rural area of Meerut and Sirmour (H.P) respectively.14,15 RTI prevalence was maximum (11.39%) in 24-29 years age group in the present study and it was similar other studies done by Pant, Sharma14,15. But Rathor et al16 reported maximum prevalence in age group of 40-49 years and Nandan et al17 reported maximum in 15-24 years age group. Significantly higher prevalence of RTI was present among women with lower literacy. The findings of the present study corroborated with the findings of the earlier studies14,15. The prevalence of RTI was maximum Cu-T users, similar findings observed by Sharma et al15 whereas it was maximum among women who had sterilization as observed by Pant et al.14 RTI morbidities was significantly higher among who used general cloths as compared to Sanitary pad and clean cloths users and it was corroborated with the findings of Sharma et al 15.
It can be concluded from the present study that community based awareness generation programme about small family norm, maintenance of reproductive hygiene through use of sanitary napkins, practice of barrier method of contraception as well as education are essential to reduce RTI Morbidities. Special emphasis should be made to involve local quack practitioners about RTIs/STIs for early referral to higher health facility. So for quack practionars training programme should be arranged for early identification and referral of the patient by syndromic approach.. IEC activities need to be strengthened through mass media and interpersonal communication starting from grass root to tertiary care level.
References
- Syndromic management of vaginal discharge among women in a reproductive health clinic in India. Sex Trans Infect. 2000;76:303-6.
- [CrossRef] [PubMed] [Google Scholar]
- Prevention and management of reproductive infection and sexually transmitted infections, RCH Module for Medical officer of Primary Health Centre, NIHFW, New Delhi. 2000 May:467-494.
- [Google Scholar]
- Reproductive morbidity in an urban slum: Need for health Education. Sex Transm Infect. 2002;78:68-9.
- [CrossRef] [PubMed] [Google Scholar]
- High prevalence of gynaecological diseases in rural Indian women. Lancet. 1989;1:85-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of clinically detectable gynaecological morbidity in India: Results of four community based studies. Journal of Family Welfare. 1997;43:8-16.
- [Google Scholar]
- Management and Control of RTIs including STIs: NACO Module. New Delhi: Ministry of Health and Family Welfare, Government of India; 2007. p. :1.
- [Google Scholar]
- Reproductive tract infections among rural women in Merrut. Indian J Med Sci. 1999;53:359-60.
- [Google Scholar]
- Vaginal discharge: Its causes associated symptoms as perceived by rural North Indian Women. IJCM. 2007;32:22-6.
- [CrossRef] [Google Scholar]
- Screening for STDs in rural women in Papua newguinea: Are WHO therapeutic algorithms appropriate for case detection. World Health Organisation. 1998;76:401-11.
- [Google Scholar]
- Estimation of prevalence of RTIs/ STDs among women of reproductive age group in Agra district. J Med. 2002;37:110-3.
- [Google Scholar]
- Community based study of reproductive infections among ever married women of reproductive age in a rural area of Haryana. Ind J Community. 1999;31:223-8.
- [Google Scholar]
- Prevalence of vaginal discharge in a urban slum of Chandigarh. Med Yezettee. 1994;138:431-2.
- [Google Scholar]
- Efficacy of syndromic approach in management of RTI and associated difficulties in rural area of Chandigarh, IJCM. . 2002;27:110-3.
- [Google Scholar]
- Social correlates in RTIs among married women in rural area of Meerut. IJCM. 2008;32:52-3.
- [CrossRef] [PubMed] [Google Scholar]
- The prevalence of RTIs and STDs among married women of reproductive age group in a rural area. IJCM. 2009;34:62-64.
- [CrossRef] [PubMed] [Google Scholar]
- Improving reproductive health and family spacing in the state of UP “A socio-clinical study by RTI / STD cases. CARE India 1997
- [Google Scholar]
- Vaginal Discharge, Perceptions and health seeking behaviour among Nepalese women. J. Pak Med. Association. 2004;54:620-4.
- [Google Scholar]




