
Translate this page into:
Assessment of Breakthrough infection among people diagnosed with COVID-19 Infection at Tertiary Care Hospital in Rishikesh: A cross-sectional study
CORRESPONDING AUTHOR: Mahendra Singh, Associate Professor, Department of Community and Family Medicine, All India Institute of Medical Sciences, Rishikesh E Mail ID: gehlot.mahendrasingh@gmail.com
-
Received: ,
Accepted: ,
CITATION: Chauhan S, Manohar A, Saini B, Singh M, Aggarwal P, Bahurupi Y. Assessment of Breakthrough infection among people diagnosed with COVID-19 Infection at Tertiary Care Hospital in Rishikesh: A cross-sectional study. J Comp Health. 2022;10(2):65-71. Doi: https://doi.org/10.53553/JCH.v10i02.004
Abstract
Background:
The second wave of Covid-19 in India declined in July 2021. A contagious variant known as Omicron variant replaced the delta variant as the dominant variant which was seen in different parts of the country in the third wave. At the same time the incidence of COVID-19 Breakthrough infections was also began to emerge and many cases were detected in due course of time.
Objective:
The present study was done to estimate the prevalence of breakthrough infection of Covid-19 (SARSCoV-2) infection in those who are fully vaccinated with either AZD1222 (ChAdOx1-S) or BBV152 vaccine and its clinical outcome among the Vaccinated beneficiary. The secondary objective is to assess the Sociodemographic and Clinical profile of people who are tested positive for the COVID-19 infection.
Methodology:
A descriptive Cross-sectional study was conducted. All People who came to the screening OPD for COVID 19 screening at AIIMS Rishikesh during 1st January 2022 till 30th March, 2022 were included and those being tested negative or didn't give consent were excluded. Systematic random sampling was used while selecting participants.
Results:
The proportion of breakthrough infection is (82.9 %) among those who are tested positive for the COVID 19 infection. Among HCWs it is 100 % and among Non-Health care worker it is 92.7 %. The symptoms in the Breakthrough infection in vaccinated people are usually milder and may result in very fewer hospitalizations. Vaccination have an obvious advantage in averting severe disease, hospitalization and deaths.
Conclusion:
This study also indicates that even after vaccination, people needs to follow COVID-19 appropriate behavior and Non-pharmaceutical interventions. The high breakthrough infection reflects that in addition to vaccination which is a critical component of the prevention measure we need to adopt multiple strategies like following the COVID-19 appropriate behavior and Non-pharmaceutical interventions. Also there should be a continuous monitoring of post vaccination breakthrough infection which should be done by all countries.
Keywords
Breakthrough Infection
COVID-19
Covaxin
Covishield
Vaccination
Variants of concern (VOC)

INTRODUCTION
Coronavirus disease (COVID-19) is an infectious disease caused by a newly discovered coronavirus. When epidemic started due to the novel strain of SARS-COV2, it quickly spread across the whole world which become a major Public Health Emergency of International concern for the whole world due to its severity and high contagious nature (1) Vaccination has been the most successful and effective measure in reducing the mortality and morbidity in the world. Once again the COVID-19 vaccination has proved its importance and effectiveness in the fight against COVID19. DCGI has approved the COVAXIN and Covishield by EUA (emergency use authorization) in India. India began its world largest vaccination drive in mid-January. It started vaccinating its people gradually starting with the Health care workers and Frontline workers. In the next phase, elderly population, people with co-morbidities, and people whose age is >45 years which is followed by the remaining proportion of population of age group (18 to 45) or less than 18 age group. According to the ICMR data the incidence rate of these cases is 0.05%.and prevalence of 0.03 % for Covishield and 0.04 % for Covaxin. (2) Since breakthrough cases are casting a shadow of doubt among people and raising question on its effectiveness, it is necessary to obtain data on the prevalence of those breakthrough infection. The third wave of the pandemic in India started in January and it continued till March 2022. The emergence of the mutation in the SARS-COV2 virus led to the spike in the number of cases. Unlike during the delta wave in 2021, this time the virus was met by a largely vaccinated adult population most adults had received either Covishield or Covaxin. In addition, many individuals had already acquired immunity through natural infection. In India, 3rd dose of the same vaccine (a homologous booster dose) was authorized for healthcare and frontline workers and for people over the age of 60, on January 10, 2022. Both of these vaccines are known to generate an immune response when they are used as a homologous booster dose. However, there is no published information available on the clinical outcomes of this intervention in the Indian context.(3)An exhaustive list of mutations of SARS-CoV-2 strains has been identified. The World Health Organization (WHO) has classified five variants as variants of concern (VOC); Alpha, Beta, Gamma, Delta, and Omicron and other WHO variants of interest (VOI) include Lambda and Mu. While there are over two dozen approved COVID-19 vaccines, the mutations in the virus topology, viral load, as well as duration of viral RNA shedding play a role in the transmission of the disease.(4)This study estimates the percentage of breakthrough infections in HCW and NHCW who are diagnosed with COVID 19 infection and received full dose of the vaccine. This study was done when the Omicron-driven third wave was winding down in India. With more waves expected in the future, and wider availability of 3rd doses now to all above the age of 18, it is important to collect pertinent information about the overall community experience during the third wave.(3)
MATERIAL & METHODS
At the Tertiary care center in Rishikesh, we identified breakthrough infections by performing critical evaluations of health care workers and Non-health care workers who were exposed and are found to be symptomatic (including mild symptoms). Patients with COVID-19 cases was identified from the Screening OPD/Covid-19 lab of AIIMS Rishikesh Systematic random sampling was used while selecting sample. A Semi structured predetermined questionnaire was prepared which includes information COVID-19 infection details, Sociodemographic details, Vaccination status details. By using the list of people who are found positive with the corona virus, an interview schedule was used to conduct telephonic interview. All the eligible participants were told about the purpose of the study and the need for asking their vaccination status and COVID-19 details. An informed consent was also obtained from them. After collecting the data, a separate list of people was prepared for the people who fulfilled the criteria of breakthrough infection and then data was be analyzed for the breakthrough infection. For Statistical Analysis data was arranged or entered in Microsoft Excel spread sheet and analyzed by using SPSS version 25 for windows. Descriptive statistics was used to present all outcomes. Binary and categorical variables were presented using counts and percentages. For Comparison of categorical variables chi square test was used. The study was approved by the Institutional Ethics Committee (AIIMS/IEC/21674). Verbal consent was obtained from the HCWs and NHCWs after informing them that the participation is voluntary, and there is no harm to the participant in our study who responded to the telephonic interviews.
Standard operating definition Breakthrough Infection:
If a person has received both doses of vaccine and have tested positive for Corona virus, after ≥14 days, such cases are referred to as breakthrough infection.
RESULTS
Table 1 -Most of them 153 (86.9%) were vaccinated. 21 people have comorbidities like HTN and Diabetes. Majority of cases were asymptomatic. Only 2 (1.13 %) patients needed hospitalization. Median duration between fully vaccination and tested positive status for COVID-19 is 138 with an IQ of 22-289.
| Characteristics | N = 176 |
|---|---|
| Age (years) | |
| Median (Interquartile range) | 30 (27-47) |
| Gender | |
| Male | 99 (56.2 %) |
| Female | 77 (43.7 %) |
| History of COVID-19 Vaccination | |
| Yes | 153 (86.9 %) |
| No | 23 (13.0 %) |
| Co-morbidity | |
| Yes | 21 (11.9 %) |
| No | 155 (88 %) |
| Profile | |
| Health Care Worker(HCW) | 58 (32.9 %) |
| Non-Health Care Worker(NHCW) | 118 (67.04 %) |
| Symptomatic during the course of illness | |
| Yes | 51 (28.9 %) |
| No | 125 (71 %) |
| Hospitalization | |
| Yes | 2 (1.13 %) |
| No | 174 (98.8 %) |
| Time Interval between COVID-19 vaccination and tested positive for COVID-19 (In days)* | |
| Median (Interquartile range) | 138 (22-229) |
Table 2 -COVID-19 cases with vaccinated individuals does not show statistically significant difference when compared with non-vaccinated COVID-19 cases in reference to Age, gender, symptom status. Hospitalization is significantly less in Vaccinated people as compare to non-vaccinated
| Characteristics | COVID19 cases with Vaccination | COVID 19 cases without Vaccination | P - Value |
|---|---|---|---|
| (N=153) | (N=23) | ||
| Age (Years) | |||
| Median(Interquartile range) | 20(27-47) | 21(27-48) | .279 |
| Gender | |||
| Male | 89 (58.2 %) | 10 (43.5 %) | .185 |
| Female | 64 (41.8 %) | 13 (56.5 %) | |
| Profile | |||
| HCW | 56 (36.7 %) | 2 (0.86 %) | .008 |
| Non HCW | 97 (63.3 %) | 21 (91.3 %) | |
| Symptomatic | |||
| Yes | 48 (31.4 %) | 18 (78.2 %) | .348 |
| No | 105 (68.6 %) | 5 (21.7 %) | |
| Hospitalization | |||
| Yes | 2 (1.3 %) | 0 | .031 |
| No | 151 (98.6 %) | 23 (100 %) |
Table 3 -There is (82.9 %) breakthrough infection among those who are tested positive for the COVID 19 infection. Many people are asymptomatic in nature and overall there are very less hospitalization (1.36)
| Characteristics | Total COVID-19 breakthrough infection (N=146) |
|---|---|
| Age (Years) | |
| Median(Interquartile Range) | 30 (27-47) |
| Gender | |
| Male | 86 (58.9%) |
| Female | 60 (41.0%) |
| Type of Vaccine | |
| Covishield | 116 (79.4 %) |
| Covaxin | 30 (17.0%) |
| Symptomatic | |
| Yes | 47 (32.1 %) |
| No | 99 (67.8%) |
| Hospitalization | |
| Yes | 2 (1.36%) |
| No | 144 (98.6%) |
| Time duration between Fully vaccination status and tested positive for COVID-19 (In days) | |
| Median (Interquartile range) | 195(123-299) |
Table 4: Comparison of COVID-19 breakthrough infection among HCW and NHCW. The proportion of breakthrough infections shows statistically significant variation only when compared with the mean duration between Fully vaccination status and tested positive for COVID-19.
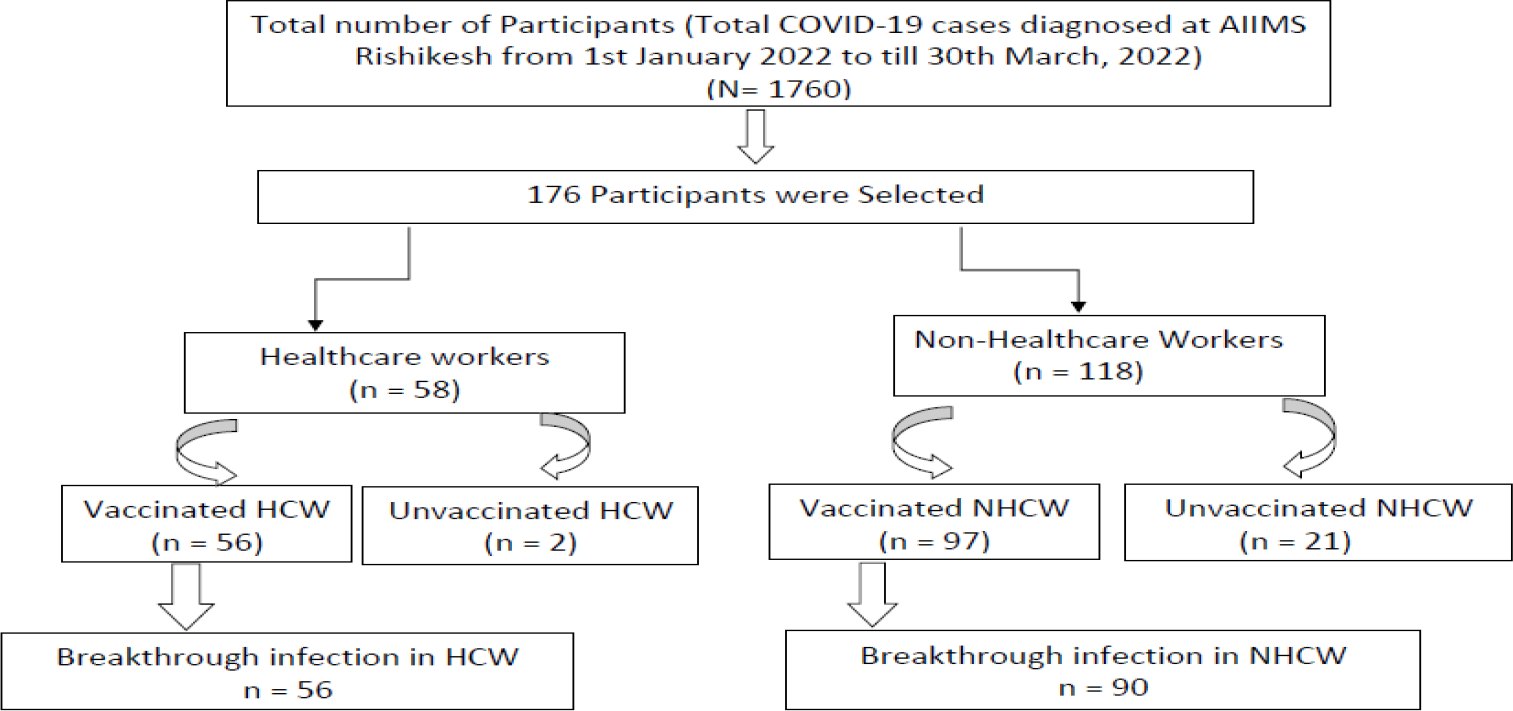
- FLOW DIAGRAM OF BREAKTHROUGH INFECTION IN THE STUDY PARTICIPANTS.
| Characteristics | HCW with COVID 19 breakthrough infection (N=56) | NHCW with COVID 19 breakthrough infection (N=90) | P value |
|---|---|---|---|
| Age (Years) | |||
| Median(Interquartile Range) | 28 (26 - 30) | 38 (28-55) | .115 |
| Gender | |||
| Male | 31 (55.3 %) | 55 (61.1 %) | .253 |
| Female | 25 (44.6 %) | 34 (37.7 %) | |
| Type of Vaccine | |||
| Covishield | 41 (73.2 %) | 75 (83.3 %) | .000 |
| Covaxin | 15 (26.7 %) | 14 (15.5 %) | |
| Symptomatic | |||
| Yes | 16 (28.5 %) | 31(34.4%) | .275 |
| No | 40 (71.4 %) | 58 (64.4 %) | |
| Hospitalization | |||
| Yes | 0 (%) | 2 (2.2 %) | .059 |
| No | 56 (100 %) | 87 (96.6%) | |
| Time duration between Fully vaccination status and tested positive for COVID-19 (In days) | |||
| Median (Interquartile range) | 278 (173 - 309) | 180 (102 - 274) | .002 |
DISCUSSION
COVID-19 vaccines are a critical tool for controlling the ongoing global pandemic. Viral variants are also emerging from the existing virus which has threatened the protection given by the vaccines and also responsible for breakthrough infections. Hence it is necessary to assess the distribution and its pattern in different part of the country. There is also limited data regarding COVID-19 breakthrough infection in Uttarakhand which needs to be studied. So, in this present study, we assessed the COVID-19 Breakthrough infection among people who are diagnosed with COVID-19 infection at Tertiary Care Hospital in Rishikesh.
Other studies revealed 67 cases (9.8%) required hospitalization and fatality was observed in only 3 cases (0.4%). The infection among breakthrough cases predominantly occurred through Delta variant indicating its high community transmission during this period followed by Alpha and Kappa variants. In our study, only 2 cases (1.36%) required hospitalization. This clearly suggests that vaccination reduces severity of disease, hospitalization and mortality. Therefore, enhancing the vaccination drive and immunizing the populations quickly would be the most important strategy to prevent further deadly waves of the COVID-19 and would reduce the burden on the health care system. Post-vaccination breakthrough COVID-19 infections have been reported from various countries with use of different licensed vaccines. It appears that the current COVID-19 vaccines are disease modifying in nature wherein mild or less severe infections are expected to occur in vaccinated individuals. However, vaccination seems to have an obvious advantage in averting severe disease, hospitalization and deaths. Therefore, continuous monitoring of post vaccination breakthrough infections along with clinical severity of disease must be adopted as an essential component of vaccine roll-out program by all countries. Such monitoring will help us to understand the need to adequately tweak the available vaccines and also develop new vaccines with enhanced potential to protect against variant strains of SARS-CoV-2 (5)
The proportion of breakthrough infection is (82.9 %) among those who are tested positive for the COVID 19 infection. Among HCW diagnosed with COVID-19 infection is 100 % and among NHCW it was 92.7% during the third wave of COVID 19. Contrary to our findings Pragya Sharma et al reported lower proportion of breakthrough infection. The rates of breakthrough infection observed in the other study conducted during April and May 2021 was 11.3% were slightly lower than that observed during surveillance in a chronic care facility in Delhi, India (13.2%) where HCWs received either Covishield or Covaxin. However, another study in a large cohort of HCWs from a north Indian city vaccinated with Covishield reported the incidence of Covid-19 breakthrough infections to be only 1.6% (48 out of 3,000) while 2.6% tested positive after receiving at-least one dose of the vaccine. In contrast, Hacisuleyman et al. report the incidence of breakthrough infection as just 0.5% in a cohort of 417 health care workers who had previously received two doses the BNT162b2 (Pfizer-BioNTech) or mRNA-1273 (Moderna) vaccine which is much lower than reported in our study (6)
Similar to our finding that more number of people with breakthrough infection receive Covishield vaccine another study reported that a higher number of fully vaccinated individuals with Covishield could have led to more breakthrough cases in individuals who received Covishield in comparison to Covaxin in the eastern state. (8)
One study reported that during second wave when Delta variant, along with Alpha, Kappa, Delta AY.1, and Delta AY.2 was circulating then Fever (69%) was the most consistent presentation, followed by body ache, including headache and nausea (56%), cough (45%), sore throat (37%), loss of smell and taste (22%), diarrhea (6%), and breathlessness (6%), and 1% had ocular irritation and redness. (5) Contrary to Nivedita Gupta et al study we found that during third wave Cough (33%) was the most consistent presentation, followed by the Runny Nose (28%), Sore Throat (24%), Shortness of Birth (8%), Fever (7%) forms the majority of the symptoms. In this study, the high rate of COVID-19 breakthrough infection may be attributed to this Omicron variant, which was dominant variant during the third wave as compared to the delta variant which driven the second wave in the country which can be confirmed by genomic sequencing analysis of all breakthrough samples. Omicron variant which is known to have a more transmissible in nature than the previously circulating strain and it is also capable of escaping prior immunity.
This study reports that the Median (interquartile range) age was 30 years (27-47), among people with breakthrough infection (5) and large number of breakthrough infection can be explained by the fact that more HCWs are getting exposed to the high risk environment. More males and age group of 30 can be attributed to the Jobs and working in the essential services such as transportation, health care and food. So this could be the one of the reason why young age group are vulnerable to the SARS-COV 2 infection. Similarly, in other study the median age (and the IQR) with the breakthrough cases after two doses was 41(30-55).
Even though a lot of effort has been made in the fight against COVID-19 in which vaccines are playing a critical role to control this pandemic, but COVID-19 breakthrough infections has been neglected resulting in an ever growing pool of the disease. To detect these infections early, contact tracing and early diagnosis needs to be prioritized especially in the vulnerable groups like HCWs who are working in an environment where risk of contracting this disease is very high. The finding indicates that non-pharmaceutical interventions should be continued by both vaccinated groups HCWs and NHCWs. So this study identifies not only the possibility of breakthrough infection but the rate of hospitalization which was found to be 1.36 % among the 176 participants, all other cases had a mild infection which shows that COVID-19 vaccine effectiveness in reducing the severity of the diseases. It not only preventing the infection but also serious illness and death. Since vaccines are not 100% effective at preventing infection, some people who are fully vaccinated will still get COVID-19. So getting themselves vaccinated is crucial to slow the spread of COVID-19 and to prevent infection by delta or other variant. This study also indicates that even after vaccination, people needs to follow the COVID-19 appropriate behavior for the protection of their closed ones. There is a possibility that the people who are immunocompromised may not build the adequate level of protection from the antibodies after their two dose of vaccine series so they must take all the precautionary measures until advised by their healthcare worker.
CONCLUSION
The COVID-19 pandemic had triggered rapid development, emergency use authorization, and unprecedented collaborative efforts from various stakeholders. Vaccination is cost-effective strategy for survival and a better quality of life for the people as well as for the revival of the economy of India. Since there are large number of breakthrough infection reported in many studies there is a need of active genomic surveillance for the new SARS-CoV-2 variants and to assess their potential to evade the immune response. The result of this study indicate the need of Continuous monitoring of post vaccination breakthrough infections along with clinical severity of disease must be adopted as an essential component of vaccine roll-out program by all countries. The efficacy and safety of COVID-19 vaccination through post-marketing surveillance is of paramount importance and requires long-term follow-up. This should account for both successes and failures, outstanding benefits, and its superiority over other types of pharmacological and non-pharmacological treatment regimens. Studies are needed nationally and globally, along with transparent sharing of data and reports among all participating companies, institutions, and nations. (9) This is mandatory for periodic evaluation and re-strategize COVID-19 management plans. These data analyses can hold the keys to the future effective public health management of COVID-19 against the different strains of COVID 19 variants.
AUTHORS CONTRIBUTION
All authors have contributed equally.
REFERENCES
- World Health Organization. World Health Organization. Available from: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccine-standardization/coronavirus-disease-(covid-19) (accessed )
- [Google Scholar]
- Both Covishield & Covaxin work, only 3-4 in 10,000 infected post vaccine, Modi Govt releases data [Internet]. The Print. 2021. Available from: https://theprint.in/health/covid-deaths-among-people-aged-70-years-and-more-slightly-higher-in-2nd-wave-govt-data-shows/643657/ (accessed )
- [Google Scholar]
- Vaccine against arteriosclerosis: an update. Ther Adv Vaccines. 2018;9(6):259-61.
- [CrossRef] [PubMed] [Google Scholar]
- Mukhopadhyay (2021). Clinical Characterization and Genomic Analysis of Samples from COVID-19 Breakthrough Infections during the Second Wave among the Various States of India. Viruses, 13(9), 1782.
- [CrossRef] [PubMed] [Google Scholar]
- (n.d.). Breakthrough infection with SARS-CoV-2 and its predictors among healthcare workers in a medical college and hospital complex in Delhi, India.
- [Google Scholar]
- Covid-19 vaccine breakthrough case investigation and reporting [Internet]. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/coronavirus/2019-ncov/php/hd-breakthrough.html (accessed )
- [Google Scholar]
- Breakthrough sars cov-2 infections among BBV-152 (COVAXIN®) and AZD1222 (COVISHIELD tm) recipients: Report from the Eastern State of India. Journal of Medical Virology. 2021;94(3):1201-5.
- [CrossRef] [PubMed] [Google Scholar]
- Strategy for covid-19 vaccination in India: The country with the second highest population and number of cases. npj Vaccines. 2021;6(1)
- [CrossRef] [PubMed] [Google Scholar]




