Translate this page into:
Risk Factors Of Young Age Hypertension : A Case Control Study
Corresponding author: Dr.Parvathy R S, MD, Community Medicine, DPH,DNB, Mphil, Clinical Epidemiology , MSc. Clinical Nutrition and Dietetics, Associate Professor (CAP), Department of Community Medicine, Government medical college, Thiruvanathapuram, drzinia@gmail.com, Mobile- 9037356908
Abstract
BACKGROUND:
The objective of the study was to assess the risk factors of primary hypertension in age group of 15 -40 years at Medical college hospital Trivandrum.
METHODS:
A Case control study was done to compare hypertensives and non hypertensives in the age group of 15- 40 years. Cases were those attending the medicine OP department in the age group of 15 - 40 years and having a BP of more than 140/90 mm of mercury on two successive readings. Those in this age group with BP < 140/90 mm of mercury were taken as controls. 50 cases and 100 controls were identified. Data was collected using a semi structured questionnaire.
RESULTS:
Factors associated with hypertension in this age group by bivariable analysis included family history (OR-3.63, p- 0.0002), current smoking habit(OR- 4.92, p- 0.004), smokeless tobacco user (OR-5.3, p- 0.01), Current drinker (OR-3.8,p-0.002). After multivariable analysis using logistic regression, family history was found to be an independent risk factor for hypertension in the young.
CONCLUSION:
Early screening for detection of hypertension among young people with family history & appropriate management are important needs of the hour.
Keywords
Young age Hypertension
risk factors
family history
Kerala
Trivandrum

INTRODUCTION
Globally cardiovascular diseases accounts for 17 million deaths a year, nearly one third of the total. Of these, complications of hypertension account for 9.4 million deaths worldwide every year. Hypertension is responsible for at least 45% of deaths due to heart disease and 51% of deaths due to stroke. [1] Globally, the overall prevalence of raised blood pressure in adults aged 25 years and over was around 40 %. [2] It is estimated that the overall prevalence of hypertension is 159.46 per 1000 population in India, which is more than twice that of diabetes. [3] In 2020 AD, 2.6 million Indians are predicted to die due to coronary heart disease which constitutes 54.1 % of all CVD deaths. Nearly half of these deaths are likely to occur in young and middle aged individuals (30-69 years).[4]
A growing number of young adults are now at risk of hypertension. [5] There is no consensus on the definition of young age hypertension. It has been defined as a condition when systolic BP is at least 140mmHg and diastolic BP is at least 90mmHg in less than 40 years of age group. Young onset hypertension usually has diastolic predominance mainly due to increase total peripheral resistance. [6]In Kerala, the prevalence of people in hypertensive state varies from 3.7% in 15-19 years to 21.0% in 35-44 years.[7] This is similar to the prevalence of hypertension in the age group of 24-32 years at 19% .[8]Another study in US, reports a prevalence of 7.8% % in age group of 18-39 years.[9] Adults 18-24 years old with high blood pressure were 28% less likely to be diagnosed during doctor visits than those 60 and older.[10] Young adults have lower awareness, treatment, and control of their hypertension compared with older adults.[9] Although treatment decision based on absolute risk reduction will favour treating middle age and elderly hypertension, in terms of long term cost effectiveness, treating the young onset hypertension optimally makes good economic sense.[6] Reducing blood pressure in young brings about a steeper reduction in cardiovascular risk when compared with older people. [11] All health promotional activities aimed at hypertension control should ideally be started in young. Identifying risk factors of hypertension in young will enable the identification of at risk groups and targeted health education and prevention and control activities. This study was done to identify the risk factors of hypertension in young.
Materials and Methods
This was a case control study to identify the risk factors of hypertension in age group less than 40 years conducted in Government medical college hospital Trivandrum, Kerala, a tertiary referral centre in South India.
Study population :
Cases were those attending the medicine department in the age group of 15 - 40 years and having a BP of more than 140/90 mm of mercury or already diagnosed as hypertensives.
Controls were those attending the medicine department in the age group of 15 - 40 years and having a BP below140/90 mm of mercury and no previous history of hypertension. Those who were critically ill and not willing to give consent were excluded.
50 cases and 100 controls were recruited during the study period of three months.
Data collection:
Data was collected using interviewer administered Semi structured questionnaire. Blood pressure ( BP ) was recorded using sphygmomanometer in sitting and supine position. Other important study variables assessed were age, sex, genetic predisposition, obesity, salt intake, saturated fat intake, dietary fiber consumption, physical activity, alcohol consumption, smoking, socio economic status, history of Cardiovascular events and associated diseases Ethical consideration: Clearance was obtained from the Institutional ethics committee. Informed written consent was taken from the subjects.
Data analysis:
Data was entered in excel sheet and analysis was done in SPSS-11 . Bivariable analysis was done using chi-square test for qualitative variables & t-test for quantitative variables. Variables which were significant in bivariable analysis were put to multivariable analysis using logistic regression. Odds ratios with 95% confidence intervals were calculated.
RESULTS
Among the cases, 27 were males and 23 were females. Among controls there were 50 males and 50 females. Among cases, 82% were previously detected hypertensives and 18% trols (table1) and hence they are comparable. were newly detected. The socioeconomic characteristics like income, education and employment status were not significantly different among cases and con 62% of cases had family history of hypertension whereas only 31% of controls had family history of hypertension. This difference was statistically significant. Current smokers, smokeless tobacco users, alcoholics and passive exposure to smoke were significantly higher in cases (table 2).
| Variables | Case(n=50) No (%) | Control (n=100) No (%) | X2 | P value |
|---|---|---|---|---|
| Income APL BPL |
23(46%) 27(54%) |
45(45%) 55(55%) |
0.013 | 0.9 |
| Education Primary Higher |
16(32%) 34(68%) |
30(30%) 70(70%) |
0.063 | 0.8 |
| Employment Employed unemployed |
32(64%) 18(36%) |
53(53%) 47(47%) |
1.64 | 0.2 |
| Variables | Case(n=50) No (%) |
Control(n=100) No (%) |
OR (95% CI) | p value |
|---|---|---|---|---|
| Family history | 31(62) | 31(31) | 3.63 (1.78-7.39) | 0.0002 |
| Current smoker | 15(30) | 8(8) | 4.92 (1.9-12.62 ) | 0.004 |
| Smokeless tobacco user | 7(14) | 3(3) | 5.3 (1.3-21.3) | 0.01 |
| Drinker (alcohol) | 16(32) | 11(11) | 3.8 (1.6-9) | 0.002 |
| Heart disease | 12(24) | 7(7) | 4.2 (1.53-11.46) | 0.003 |
| Past smoker | 3(6) | 2(2) | 3.68 (0.59-22.9) | 0.137 |
| Exposure to smoking | 12(24) | 9(9) | 3.778(1.4-9.8) | 0.005 |
On bivariable analysis, BMI, salt intake, vegetable consumption in a week and oil intake were found to be significantly higher among cases (table 3).Physical inactivity was more among cases than controls. The mean duration of brisk walking and active involvement in games were found to be significantly higher among controls (fig .1 )
| Variables | Cases | Controls | t value | P value |
|---|---|---|---|---|
| BMI | 23.70(3.17) | 21.50(2.42) | 05.87 | 0.0001 |
| No of days of vegetable intake /week | 5.60 | 6.19 | 11.31 | 0.001 |
| No of days of Fruit intake /week | 2.98 | 3.29 | 00.38 | 0.539 |
| Grams of oil consumed/ month | 431.00 | 307.64 | 2.96 | 0.087 |
| Grams of salt consumed/ month | 327.00 | 269.05 | 4.04 | 0.046 |
| No of days of Red meat intake /week | 1.92 | 1.35 | 0.44 | 0.512 |
| No of days of Fried food intake /week | 4.04 | 3.34 | 2.23 | 0.137 |
| No of days of Fish intake /week | 5.81 | 5.82 | 0.03 | 0.850 |
| No of days of chicken intake /week | 1.70 | 1.12 | 0.05 | 0.070 |
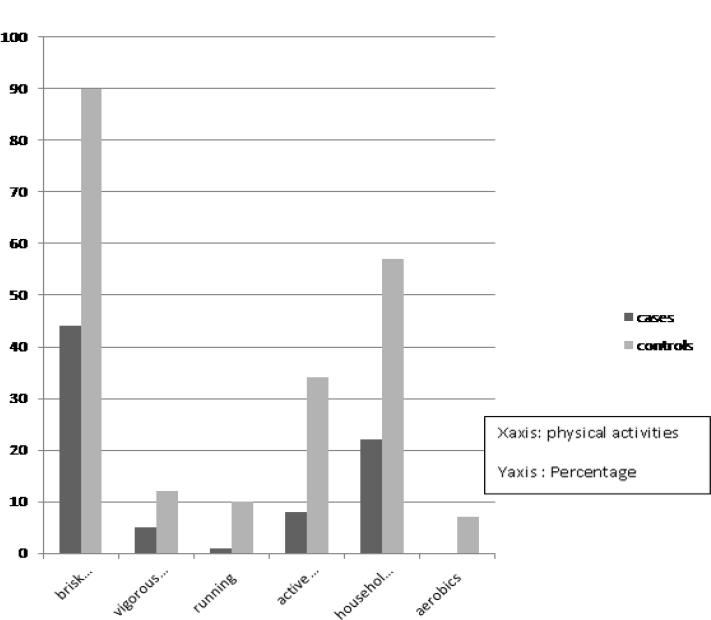
- PHYSICAL ACTIVITY AMONG CASES AND CONTROLS
On multivariable analysis, Family history was found to be an independent risk factor for hypertension in the young (p value 0.007).Among quantitative variables significant variables were oil intake & vegetable intake with p value 0.013 and 0.02 respectively.
DISCUSSION
Estimating the factors associated with hypertension in young age is important for designing strategies for the control and prevention of cardiovascular diseases. 5-10 % of hypertensives have onset at young age of 20-30 years. [12] Factors associated with hypertension in this age group by bivariable analysis in this study included family history, current smoking habit, smokeless tobacco user, Current drinker . After multivariable analysis using logistic regression, family history was found to be the single independent risk factor for hypertension in the young. These findings are similar to that obtained in another matched case control study of risk factors of hypertension in young. [13]
Genetic factors are thought to contribute by 30% -50% to the cause of essential hypertension. [14] A research conducted in Australian twins showed that heritability estimates for systolic BP was 19-56 %, and for diastolic, 37-52 %. [15] However the genes have not been specifically identified. [16]The more family members with high blood pressure before the age of 60, stronger the family history of high blood pressure. When three or more family members have hypertension, the family history of hypertension is said to be strong. [17] Compared with normotensive offspring of normotensive parents, normotensive offspring of hypertensive parents have increased blood pressure and impaired arterial properties. These differences were exhibited conspicuously in men but not in women.[18]. Normotensive young men with a family history of hypertension have vascular abnormalities that involve veins as well as arteries.[19]
Women with family history of hypertension may have greater sympathetic reactivity compared to those with a negative family history.[20] Individuals with two hypertensive parents had high insulin, insulin resistance and low- density lipoprotein cholesterol. Women with two hypertensive parents had higher systolic BP and diastolic BP during waking and sleep periods. In men it was related only to higher diastolic BP during waking.[21] While managing young onset hypertension, those with a strong family history most likely have essential hypertension. Those without family history should be investigated for secondary hypertension. Hypertension, which is mainly systolic, could be spurious systolic hypertension of the young.[6] A family history of Hypertension significantly predicts the future onset of disease, although the strength of prediction also depends on sex , age, degree of relation and the number of family members affected.[16]Type A behaviour, social desirability and introversion differentiated 17-39 year old males with elevated casual systolic blood pressure from normotensive controls, in addition to the known predictors of BMI and family history. [22]
Although all lifestyle modification must be repeatedly emphasized in young, because it is theoretically more easily implemented in this age group, cessation of smoking, alcohol abstinence and weight reduction are probably more effective than salt reduction in the young. [6]Tobacco is a known risk factor for hypertension. The mean age of initiation of smokeless tobacco use was 18 years in Mizoram and 20 years in rest of the states in India among young respondents (15-34 years). The prevalence of use of smokeless tobacco in young age in the state was low (2.3-4.1%). Current smoking prevalence ranged from 1.1% to 18.6% in age groups 15- 44 years in the state.[7]
The mean age of initiation of alcohol among the younger age group (15-34 years) was 20 years in Andhra Pradesh and Madhya Pradesh, 22 years in Kerala and 21 years in rest of the states. Prevalence of alcohol use varied from 4% to 12% in the various states of India. In Kerala in the age group of 15 -44 years it varied from 5.6% to 24.3%.[7] These point towards the need for reinforcing the strategies aimed at cessation of tobacco and alcohol use in order to prevent early onset of hypertension. Intervention studies and reviews on the effects of intentional weight loss studies have reported that moderate weight losses (losses of 5% to 10%) are associated with significant improvements in hypertension. [23,24]
A review of randomized control trials reported a diastolic reduction of 0.92 mm Hg per kilogram of weight loss.[25] The weight/hypertension relationship is complex and needs well-conducted studies with long-term follow-up to examine the effects of weight loss on hypertension outcomes. [26] The prevalence of overweight in Kerala increased from 12% in 15-24 age groups to 34% in 35-44 years. [7] It is important to target weight reduction strategies in the young and it can be a part of the National Programme for Control of Cardiovascular disease, Diabetes, Cancer and stroke (NPCDCS) in India.
Adequate evidence is available, from studies conducted within and across populations, to link several nutrients, minerals, food groups and dietary patterns with an increased or decreased risk of CVD. [27] Fiber consumption predicted insulin levels, weight gain and cardiovascular risk factors like blood pressure, plasma triglycerides, LDL and HDL cholesterol and fibrinogen more strongly than other dietary components in the CARDIA cohort study of young adults (CARDIA).[28] Dietary fats associated with an increased risk of CHD include trans-fats and saturated fats, while polyunsaturated fats are known to be protective. Dietary sodium is associated with elevation of blood pressure, while dietary potassium lowers the risk of hypertension and stroke. Regular frequent intake of fruits and vegetables is protective against hypertension, CHD and stroke. Composite diets (such as DASH diets, Mediterranean diet, ‘prudent’ diet) have been demonstrated to reduce the risk of hypertension and CHD.[27] The mean number of days of consumption of fruits is lesser at 2.9 days in the state when compared to vegetables (5.5 days). 87.3% of the population took less than the adequate number of servings of fruits and vegetables. This situation would not be much different or rather worse in younger age groups. [7]
It is shown that young adults who devote more time to physical activity have a reduced risk of developing high blood pressure in the next 15 years. [29] Few studies have estimated the physical activity levels in Indian population.[4] 76% of people of Kerala have low physical activity. [7] In US about 14 percent of young people report no recent physical activity. Inactivity is more common among females (14%) than males (7%). [30] Physical inactivity starts from school as modern day teaching hardly stresses the importance of physical education. Eighty per cent of our young population is physically inactive. Even those who did exercise concentrate on muscle building rather than aerobic training.
Youngsters have to undertake aerobic physical activity for 30-60 minutes a day for at least five days a week. [31]
People aged 18-31 have a 33% slower rate of hypertension diagnosis compared with adults aged 60 or older. They are also less likely to have received counseling on lifestyle modifications. [32] Young adults have limited understanding of hypertension and it varied with hypertension risk status and gender.[33] These underscore the need for comprehensive and revitalized health care system interventions for the control of risk factors of hypertension tailored to the needs of young adults, which have been identified in this study . Early screening for detection of hypertension among young people with family history & appropriate management are also important needs of the hour.
Acknowledgement :
We express our deepest sense of gratitude to Prof.Dr.Vijayakumar, Head of the Department of Community Medicine for his guidance, support and help for doing this . We thank Dr D Dalus Professor & Head, Department of Internal Medicine, Medical College Hospital, Trivandrum for permitting us to do the project. Our gratitude is also due to our dear principal Dr.Ramdas Pisharody for facilitating such works in the institution.
References
- Raised Blood Pressure, Situation and Trends. Available at http://www.who.int/gho/ncd/riskfactors/blood pressure prevalence text/en/ (accessed )
- [Google Scholar]
- Diabetes, Cardiovascular Disease and Stroke (NPCDCS).A manual for Medical Officers. Developed under the Government of India - WHO Collaborative Programme. 2008-2009
- [Google Scholar]
- Supported by Ministry of Health & Family Welfare, Government of India and World Health Organization. Available at http://www.searo.who.int/india/topics/cardiovascular diseases/NCDResourcesNationalCVDdata base-FinalReport.pdf?ua=1 (accessed )
- [Google Scholar]
- NIH Medline plus. Available at http://www.nlm.nih.gov/medlineplus/magazine/issues/fall11/articles/fall11pg10-11.html. (accessed )
- [Google Scholar]
- Management of Young Onset Hypertension. Available at http://www.msh.org.my/filedir/1099634813474f742791327.pdf. (accessed )
- [Google Scholar]
- Indian Council of Medical Research (ICMR), 2009,IDSP Non-Communicable Disease Risk Factors Survey, Phase-I States of India, 2007-08. National Institute of Medical Statistics and Division of Non-Communicable Diseases, Indian Council of Medical Research, New Delhi, India
- [Google Scholar]
- National Longitudinal Study of Adolescent Health (Add Health), 1994-2008. ICPSR21600-v15. In: Inter-university Consortium for Political and Social Research [distributors]. Chapel Hill, NC: Carolina Population Center, University of North Carolina- Chapel Hill/Ann Arbor, MI; 2014. http://doi.org/10.3886/ICPSR21600.v15
- [CrossRef] [Google Scholar]
- Available from: http://www.cdc.gov/nchs/data/databriefs/db133.htm (accessed )
- Hypertension Newsletter. 2013 February 15 Available at http://www.health24.com/Medical/Hypert ension/News/Hypertension-in-young- adults-often-undiagnosed-20130210 (accessed )
- [Google Scholar]
- Strategies for initial management of hypertension. Indian J Med Res 2010 November 132:531-542.
- [Google Scholar]
- Hipertensi : Definisi, Prevalensi, Farmakoterapi, dan Latihan Fisik. Cermin Dunia Kedokteran. 2009;36(3):161-167.
- [Google Scholar]
- Risk factors of essential hypertension in young adults in banyudono sub district boyolali district. Available at http://www.phgmu.org/test/wisuda/publik asi/online/foto_berita/herbertwau.pdf, (accessed )
- [Google Scholar]
- Hypertension Principles and Practice. USA: Taylor & Francis Group, LLC; 2005.
- [CrossRef] [Google Scholar]
- Heritability and stability of resting blood pressure in Australia twins. Twin Res Hum Genet (9):205-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pérez Fernández, Merlin Garí Llanesc, Vielka González Ferrerd, Beyda González Camachod, Francisco L. Moreno- Martínez et al. Factors associated with prehypertension in young adults between 20 and 25 years of age. CorSalud (1):25-35.
- [Google Scholar]
- Available at http://www.cdc.gov/pcd/issues/2005/apr/pdf/04013401.pdf. (accessed )
- Family history of hypertension and arterial elasticity characteristics in healthy young people. Hypertens Res. 2008;31(5):l833-9. doi: 10.1291/hypres.31.833.
- [CrossRef] [PubMed] [Google Scholar]
- Venous abnormality in normotensive young men with a family history of hypertension. Hypertension. 1986;8(2):142-6.
- [CrossRef] [PubMed] [Google Scholar]
- Sympathetic reactivity in young women with a family history of hypertension (680.11) FASEB J 2014 Apr2 1(1 Supplement):680-11.
- [CrossRef] [Google Scholar]
- How family history and risk factors for hypertension relate to ambulatory blood pressure in healthy adults. J Hypertens. 2008;26(2):276-83.
- [CrossRef] [PubMed] [Google Scholar]
- Personality traits in young males at risk for hypertension. J Psychosom Res. 1982;26(6):585-9.
- [CrossRef] [PubMed] [Google Scholar]
- Reduction in incidence of diabetes, hypertension and lipid disturbances after intentional weight loss induced by bariatric surgery: the SOS Intervention Study. Obes Res. 1999;7:477-484.
- [CrossRef] [PubMed] [Google Scholar]
- Intentional weight loss: Patterns in the general population and its association with morbidity and mortality. Int J Obes Relat Metab Disord. 1997;21(suppl 1):S14-S19.
- [Google Scholar]
- Influence of weight reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2003;42:878-884.
- [CrossRef] [PubMed] [Google Scholar]
- John Broom Effects of Weight Loss in Overweight/Obese Individuals and Long-Term Hypertension Outcomes A Systematic Review. Hypertension. 2005;45:1035-1041.
- [CrossRef] [PubMed] [Google Scholar]
- Diet, nutrition and the prevention of hypertension and cardiovascular diseases. Public Health Nutrition. ;7(1A):167-186. DOI: 10.1079/PHN2003587
- [CrossRef] [PubMed] [Google Scholar]
- Dietary fiber, weight gain, and cardiovascular risk factors in young adults. Journal of the American Medical Association. 1999;282:1539-46.
- [CrossRef] [PubMed] [Google Scholar]
- " Science Daily. Science Daily, 21 March 2007. Available at www.sciencedaily.com/releases/2007/03/070320110911.htm. (accessed )
- [Google Scholar]
- Adolescents and Young Adults. A Report of the Surgeon General. U.S. Department Of Health And Human Services. Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion. The President's Council on Physical Fitness and Sports Available at http://www.cdc.gov/nccdphp/sgr/pdf/adoles.pdf (accessed )
- [Google Scholar]
- Attention young India, take care of your heart. IST IST 2013 December 15:00-14. http://www.thehindu.com/opinion/open-page/attention-young-india-take-care-of-your-heart/article5460388.ece. (accessed )
- [Google Scholar]
- Undiagnosed hypertension among young adults with regular primary care use. J Hypertens. 2014;32(1):65-74.
- [CrossRef] [PubMed] [Google Scholar]
- Morton, Hypertension Views Of Young African Americans. Ethnicity & Disease. 2009;19:28-34.
- [Google Scholar]




