
Translate this page into:
Public Health and Social Measures in the Context of COVID-19 – An Online Study of Households in Kolkata and Nearby Districts of West Bengal
Corresponding author: Dr Bandana Sen, Director Professor and Head Department of Statistics, 110, C R Avenue, All India Institute of Hygiene and Public Health, Kolkata- 73, E mail Id: vandanadasgupta@gmail.com
Abstract
Introduction:
COVID-19, the disease and "lockdown", the preventive measure, can be termed as major watershed of our times as never before in human history human lives and activities have been halted to such a huge level as combat measure against any disease. Under this unprecedented situation, an online survey was conceptualised to see the situation of students' households during lock down period.
Objective:
On the basis of that data, feasibility of adherence regarding public health aspects (like washing hands, physical distances, and restricted movement outside house) are discussed through this study. Moreover, the awareness, capability and feasibility of households to abide by the prescribed norms are numerically measured through related social variable and logical insight.
Method:
Though this cross sectional survey data collected during May 15 to May 31st 2020, three separate indices regarding three major points of guideline e.g. Frequent hand washing, keeping physical distance and staying inside home are devised and finally a composite normalised index is created to judge the overall status of the households.
Results:
This composite index is robust and sensitive enough. It is found to related with the level of living of the households, household size and some other social parameters.
Conclusion:
Respondent households being mostly from Kolkata nearby areas (Howrah, Hooghly, 24 PGS (N) &(S)) of Hindu, General and largely (two-thirds) belonging to 'lower-middle class' (family income per month 15000 or less) can be very well assumed as a representative sample of whole west Bengal. With the help of this composite index we may identify the status of any household in the spectrum of plausibility to adhere the guidelines and public health educative measures can be taken for those households in the long run.
Keywords
Online Survey
Lockdown
COVID 19
Index of Lockdown.

Introduction :
In December 2019, the news of the spread of COVID-19 in China came into the public domain. In India, neither there was any perceived severity of the disease nor there was any declared specific preventive measure till March. The Government of India on March 22, 2020 ordered a voluntary curfew followed by a number of combat regulations in different phases completely limiting the movement of above 1.3 billion population of the land as a preventive measure Not a single individual is spared either from its direct or indirect impact almost. In this paper attempt has been made to focus on some of these changes from the responses of an online survey, with special reference to student community.
In such a hard time stringent obeyance of lockdown rules definitely is of utmost importance and it is also necessary to know how the different categories of citizens are adjusting themselves in this unprecedented situation. Thus, an online survey was undertaken to study the conditions of the students' and to assess their situation. Phase IV of "lockdown" has been selected as the timeframe. The online survey was conducted with current students of five colleges viz. Banipur Mahila Mahavidyalaya of 24 Pgs(N), Bijoy Krishna Girls' College of Howrah Maulana Azad College, St Paul's CM College and Women's Christian College of Kolkata during 15th to 31st May 2020. As this was an online survey, having internet connection was a mandatory precondition.
Methodology:
There are series of guidelines from the central and the state governments as well as from ICMR and WHO for the prevention of interpersonal spread of this highly contagious disease. Side by side the "Dos & Don'ts" of the rules have generated huge panic in the society. The WHO guidelines to protect an individual from the spread COVID-19 suggest the following precautions:
One has to regularly and thoroughly clean hands with an alcohol-based hand rub or wash them with soap and water.
One has to maintain at least 1 metre (3 feet) distance from others.
One has to avoid going to crowded places.
One must avoid touching eyes, nose and mouth.
One has to follow good respiratory hygiene.
The suggested points above may be summarised as (i) Frequent hand hygiene (ii) Physical distancing and (iii) Environmental hygiene at home. The data collected through this survey are used to judge how often or not the households are in a position to follow these practices.
A. Frequent hand washing:
One of the most crucial protective measures is the frequent washing of hands with soap. The mixture of soap and water accompanied by the thorough rubbing of hands kills the virus within seconds - the consensus appears to be that 20 seconds is the minimum amount of time needed. But for a large section of India's population this is easier to preach than practice. Only 50% of rural Indians and 80% of urban Indians use soap and water to wash their hands, according to the National Family Health Survey (NFHS) 2015-16. The newly rechristened ministry of Jal Shakti revealed last year that 82% of rural households and 60% of urban households don't have access to piped water. According to the National Sample Survey (NSS) 76th round report about 42% of households in rural and urban India access water through public taps, tube-wells, hand pumps located in common areas. With this survey we have tried to determine the extent of possibility to follow this measure.
The survey shows that around 73% households have the source of water inside their premises (either with piped water line or tube-well or bore-well). So 27% had to move outside to collect water. It also depicts that dependence on sources outside premises is more for households who are lower in the income category. It can be commented that frequent washing of hands is very unlikely for them.
Moreover, data on sufficiency of water were also collected, and it shows that lower the economic class there is less availability of water. More than one third of households do not have source of sufficient water; for poorest class it is nearly 50%. The sufficiency level increases to a considerable extent as we move up in the economic ladder. Among the highest income band under survey, 85% households enjoy sufficient water supply. If we look into this issue with reference to the source it shows that even with piped water inside premises, Wss = ΣaiYi i = 1, 2 with Σai = 1. of water, this proportion doubles if it is tube-well/bore-well inside premises.
Combining these two, we propose a composite index WSS viz. Index of Water Availability, which is a linear combination of two characterising variable related to water viz. Source as quality and Sufficiency as quantity. This index 'Wss' is derived as follows:
Y1= Sufficiency variable and Y2=Source variable
Data were collected in 5 point Likert's scale for Y1 and for Y2 there were 5 codes starting from good quality and convenient source to bad and collectable from outside (please refer reference no. 4 for details).
So 1 ≤ WSS ≤ 5, and because of the code structure followed, lesser the value of WSS, worse is the condition of the household regarding availability of water and in turn to follow washing measure to combat COVID19.
Results:
Table 1 below shows the distribution and proportion of these 2088 household on the basis of their WSS value. For this calculation higher weight (0.75) is given to the sufficiency variable and lower (0.25) weight is given to source variable. Among these 2088 respondent households 40% have low or just enough Water Availability Index while 5% of them are of very low status. On the other hand around one fifth of the households are enjoying ample and quantity of water with quality. If we examine this index vis-à-vis level of living of the households, it can be shown that about 50% within poorest echelon of the respondent household are in a stringent status of water availability.
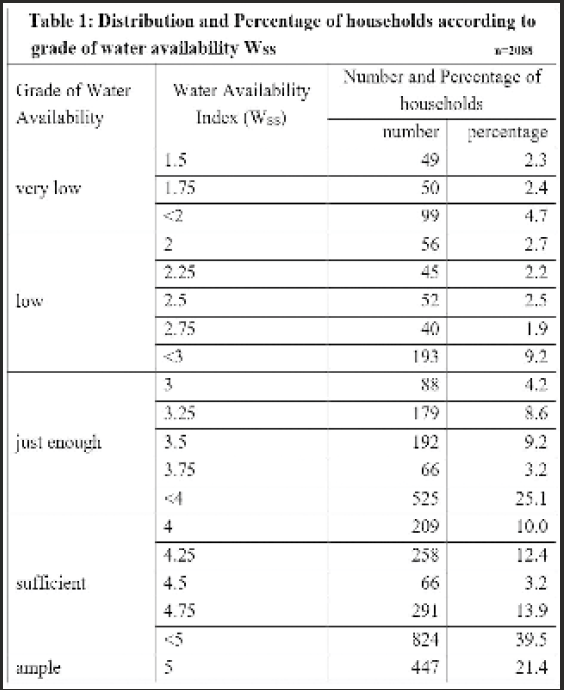
In short, access to water in India is an acute problem which gets even more severe in the country's dense settlements. Among some of these respondent households also supply is sporadic, inadequate and those who don't have access to water in their dwellings have to go out to collect water and resultantly, physical distancing is not easy to follow.
B. Physical distancing at home:
As a prescription to combat COVID19, many guidelines are issued from different quarters to "stay back home" But, in India, there's also the matter of overcrowding. An average Indian family has (approximately) five members and 40% of all homes - that is, 100 million homes - have only one room, as NSS 76th Round data suggests. In India, it is a privilege to be able to maintain physical distancing when most of the population is huddled up five to six in a room. Through this survey some data are collected in such a way that some assessment of congestion can be done as a measure of physical distancing at home.
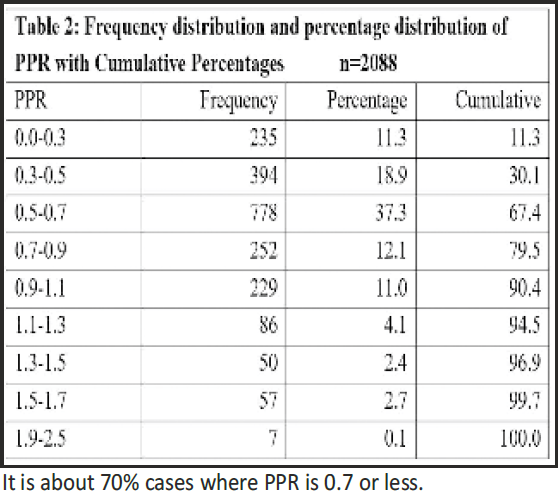
In 52% households surveyed, there are two rooms or less in the house. Thus it is important to derive PPR (Room per person) as a ratio of number of rooms to household size to see the congestion inside the room. Average value of PPR is 0. 65 ± 0.34. If we arrange this PPR in terms of frequency table the extent of congestion would be evident.
C) Environmental hygiene at home:
In this environmental hygiene we have focussed on the number inward and outer movement of non-household members and household members. This is defined by number of times a household member has gone out of house to procure (purchase or collect) food. By non-household members actually we want to assess the entry of maids and other domestic help providers predominantly as it increases the probability for infection, particularly among people with lower immunity level. Table 3 below shows such numbers.
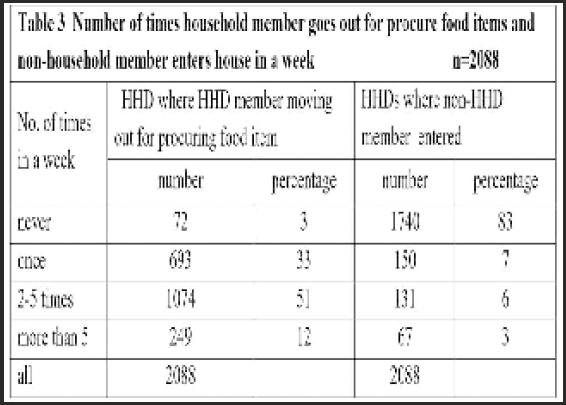
Among these three basic measures discussed so far, this is however, is in a better shape where in as high as 83% households no non-household members entered. But outward movement is not seen to be restricted as only 36% households could manage procuring food by going out only once in a week. Rest 64% had to take recourse to more frequent outward movement. But this number is assumed to be affected by many dynamics like level of living (lower echelon of the society cannot store food items for several reasons), congestion inside the house, frequent domestic clashes and many more. This unprecedented indoor confinement may result in enormous stress and uncertainty, which could take an unprecedented toll on mental health around the world, and India is no exception. Experts expect a spike in cases of anxiety and depression, as a consequence. In this survey, as already mentioned, students were the respondents, and we tried to touch upon some issues of their mental health.
Now, attempt has been made to derive a unique measure from simple household information to grade a household in the spectrum of possible agreement of Lockdown measures. From public health perspective this is important, as through simple calculation it is possible arrive at a decision whether they need any extra support to combat any such unprecedented situation.
In this index some simple information of the household will be used viz. (i) Household size say N, (ii) Number of Rooms in the Households (except veranda, kitchen, bathroom, and store room) say R, (iii) Source of water say W (iv) Sufficiency of Water Say SW, (v) household member entered the house say (iv) and (vi) number of Times one Member Needs to Go Out to Procure Food items say OMF The value of codes in the structure of IM and OMF is never as 4, once as 3, twice to 5 times as 2 and more than five times as 1.
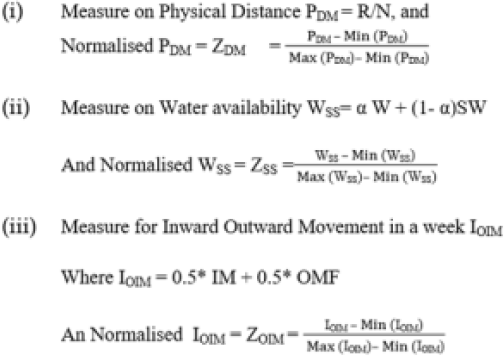
Now some derived variables (and their normalised values) are devised
Combining these three with equal weight we may derive at an Index of Lockdown as ILD where ILD
ILD can have values between 0 and 1. Now because of code structures higher the value of ILD, better is the position of the households in terms of the awareness and being equipped in combating COVID 19 through lockdown.
Table 4 below shows a distribution of Index of Lockdown applied to these whole respondent households. It vividly portrays that about 36% of the households have ILD value less than 0.4, which can be termed as very bleak as the surveyed households are primarily from urban or semi urban areas and belong to lower middle class (with at least one member is carrying out their graduation), and not urban ultra poor. Moreover, very high value (more than 0.8) is recorded for only 14 households, which is really miniscule in nature. For about 73% of the households, however, ILD is recorded as somewhat between 0.4 to 0.6.
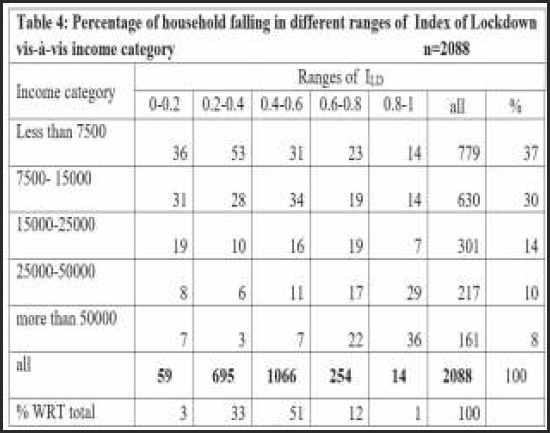
On the other hand if we see this with respect to Income category of the respective household, it portrays that while 67% and 80% of the households having ILD less than 0.2 and between 0.2 to 0.4 respectively, belong to the poor segment (income less than 15000 per month) whereas around two third of the households which have higher ILD (more than 0.8) belong to the upper echelon of the society.
Discussion:
A survey among 131 teachers of the JNU who taught online classes was carried out by professors Sood A and Kidwai A through online circulation over five days, with only those teachers who were teaching a course assigned in Winter Semester. Their theme of the study being online classes and related problem, and the results4 published by present authors were similar to their report5. However, in this study by JNU, professors were aimed at and not students and moreover no social or economic data were collected. In another similar work9 by N. Kapasia N et al, where impact of lockdown on learning status of undergraduate and post graduate students was discussed, the results regarding online classes, their devices used and relating issues are similar to our report5. However, our result on social and economic variable is the first of its kind and thus could not be compared with any other published paper/report.
From the previous section as analysed, it may be concluded that proper household infrastructure and access to water, the basic existential necessities are not easily available for many. Naturally the issue of wellbeing for those are not adequately taken care of. As this ILD is devised as a function of different household parameters (observed values of some social and housing related variables), it is completely explained by those variables. But it is also equally important to know why and to which extent these social variables are affected by other variables, most importantly, the level of living. Regression results suggest that level of living has considerable effect on this ILD. Other such important variables are household size, education status and occupation of the prime earner of the household. As a matter of fact, routine activities got severely limited, communities also adapted in creating resources and processes that enable their members to follow inconvenient rules and restrictions over unknown lengths of time.
While lock downs ensure greater adherence to the physical distancing required to break the chain of infection, inconveniences and enforced restrictions are often evaded without the 'community approach' infusing the humanising touch and sense of solidarity. The community approach requires 'social bonding', with mutual support groups being formed for people to help each other and find solutions collectively. For instance, this social bonding can ensure that basic supplies are made available to those unable to move out. It is evident that, physical distancing is possible only for the better-off: not so for the nearly 4% homeless and 40% households of India living in one-room houses (Census 2011), or for the majority who cannot stay off work, in a country where over 90% are dependent on the informal sector for livelihoods. The lockdown inevitably disrupts economic activities and livelihoods that hit the poor first and the hardest. The poor with no savings, daily wagers who earn their bread daily, informal sector and contractual workers, vendors, and so on are all going to suffer loss of livelihoods with consequent increase in child malnutrition, adult destitution and starvation, rise in other diseases and deaths. This has to be dealt with as social responsibility, with a sense of solidarity.
Conclusion:
An important aspect of the public health strategy to deal with epidemics is communication. The government must communicate with the general public and health personnel on the latest virus outbreak. The government must have a nodal person who coordinates with the health ministry/department and can provide the relevant data and advice. This is lacking at present, and, as a result, the media often sensationalises the problem, making citizens anxious. In the absence of authentic information, social media becomes the main source of information and misinformation.
Acknowledgement:
Principals of the 5 colleges where the study was carried out.
Conflict of Interest:
None
Source of Funding:
None
References:
- a pandemic lesson by Arman Bidarbaktina, Statistician, ESCAP Statistics Division; Statis Brief, UNESCAP. . 2020;23
- [Google Scholar]
- Overview of public health and social measures in the context of COVID-19. Interim guidance of WHO 2020 May 18
- [Google Scholar]
- Sanitation, Hygiene and Housing Condition In India, NSS 76th Round (July -December 2018), MoSPI, Government of India.
- [Google Scholar]
- Collaborative Project Report of Department of Statistics, AIIH&PH. (http:// www.spcmc.ac.in/)
- [Google Scholar]
- The Winter Semester of JNU Teachers' Discontent. by Ayesha Kidwai and Atul Sood (www.Jnu.ac.in)
- [Google Scholar]
- A survey based approach (digitallearning eletsonline.com) by Monica Koul and Jyoti Bhola.
- [Google Scholar]
- Students' role to look at problems in education system during lockdown issues in Maharashtra, India, by V.R. Jadhav et al. International Journal of research and Review. 2020;7(5):328-331.
- [Google Scholar]
- real-time data on children's experiences during home learning, Briefing Note BN 288, Institute for Fiscal Studies. (ifs.org.uk)
- [Google Scholar]




