
Translate this page into:
Ocular morbidity pattern and its risk factors: A study among rural population of West Bengal
Address for correspondence: The Editor/ Managing Editor, Journal of Comprehensive Health, Dept of Community medicine, NRS Medical College, 138, AJC Bose Road, Kolkata-700014
Corresponding author: Dr. Indira Dey, Dept of Community Medic, NRS Medical College, Kolkata-700014 e-mail - indiradeypal@rediffmail.com, Mobile: 9830621012.
Abstract
Background:
Visual impairment resulting from infectious diseases has declined by public health efforts but cataract and refractive errors still continue as major causes of blindness. Moreover, ageing & life style diseases also contribute to large number of blindness.
Objective:
This study was undertaken to assess the ocular morbidity pattern and the risk factors among rural population of West Bengal.
Material & Methods:
A community based, descriptive, observational study was conducted in Hariharpur PHC. One subcentre was chosen purposively and three villages under the subcentre were chosen randomly. The study population comprised of all persons residing in those villages for at least one year. Door to door visit was conducted for screening of eye problems and then detailed examination was carried out in the PHC by ophthalmic assistant. Subjects requiring specialist consultation were referred.
Results:
Difficulty with vision was the commonest complain followed by watering, burning and itching sensation, pain and redness. Refractive errors (myopia & hypermetropia) were the commonest morbidity among all age groups followed by cataract and allergic conjunctivitis. Cataract was found to be significantly associated with diabetes and hypertension (P=0.001) and allergic conjunctivitis was associated significantly with hypertension (P=0.007). Interestingly quite a high proportion of the patients with visual complaints could be detected and managed at the PHC level. So simple screening for eye disorders and utilization of trained ophthalmic assistants can enable early detection of eye conditions, prompt treatment and early referral.
Keywords
ocular morbidity
cataract
ocular morbidity
refractive errors
visual impairment.

Introduction:
According to the estimates of WHO, in 2010, 285 million people were visually impaired worldwide, of whom 39 million were blind. Developing & low-income setting countries contribute about 90% of the visual impairment.(1) In 2013, the World Health Assembly approved the 2014-19 Action Plan for the universal access to eye health with the aim of achieving a measurable reduction of 25% of avoidable visual impairments by 2019.(2)
Compared to the previous records the number of people with visual problems from infectious diseases has reduced in the last 20 years. Significant progress in preventing and curing these diseases have been achieved in many countries by concerted public health efforts.(3) However, cataracts still remain the major cause of blindness in middle- and low-income countries followed by the uncorrected refractive errors leading to moderate and severe visual impairment. In South East Asia, 50-80% of the blindness is due to cataract. Around 62.6% of blindness in India is due to cataract.(4) Age-related blindness is increasing throughout the world, as is blindness due to uncontrolled diabetes. About 80% of visual impairment can either be prevented or cured.(1)Visual impairment & blindness not only increases the burden of morbidity, it also has socio-economic implications.(5)
Population growth and increase in life expectancy are steadily increasing the number of visually disabled.(6) Life style diseases like diabetes and hypertension further complicates the scenario especially affecting the productive age group. Many of the trivial problems remain underreported ultimately leading to blindness.
High prevalence of blindness from refractive error in a community suggests that eye care services in that population are inadequate(7). Treatment of refractive error and other common morbidities should be available at the primary level of health care to reduce the burden of tertiary hospitals. Strategies such as vision screening programmes should be taken up to detect individuals suffering from visual impairment. People with low vision are to be made aware about the necessity to seek health care services for prevention of blindness. So this study was undertaken to assess the ocular morbidity pattern and the risk factors among rural population of West Bengal.
Material and Methods:
A community based, descriptive, observational study was conducted in Hariharpur PHC which falls under the rural field practice area of NRS Medical College, during a period of three months from September to November 2016. One subcentre was chosen purposively and three villages under the subcentre were chosen randomly. The study population comprised of all persons residing in those villages for at least one year who gave their verbal consent to participate in the study and were present at their house during initial screening. For minors, consent of guardian was taken. First, a door to door visit was made to screen for eligible persons with any symptomatic eye complaints or uncorrected eye diseases. If they responded affirmatively, they were asked to attend the nearest Hariharpur PHC with a referral card. 3 repeat visits were made to include all unavailable persons during the home visits. Total of 356 persons were thus identified of which 298 persons finally attended the PHC during the study period. At the PHC data collection was done using a pre-designed and pre-tested questionnaire on socio-demographic variables, other possible risk factors like addiction to alcohol or tobacco consumption, cooking fuel used, duration of television viewing, medical history etc. Visual examination for ocular morbidity was done by an ophthalmic assistant and Medical Officer of the PHC. Each eye was examined separately. Ophthalmic examination was done with the help of torchlight, magnified loop and direct ophthalmoscope. Visual acuity was assessed using standard Snellen charts. Digital tonometry was carried out and Confrontation test was done to detect any gross diminution of field of vision in cases suspected to have glaucoma. The eyeball, eyelids were examined manually and diagnosis was done clinically. Anterior segment was examined by torchlight and magnifying loop. Lastly, direct ophthalmoscopic examination of all the screened patients was also done. The data was entered and analyzed using MS Excel and Epi Info 7 and expressed as proportions. Statistical association was done using chi- square test.
Permission to conduct the study was obtained from the Institutional Ethical Committee of NRS Medical College, Kolkata. Verbal informed consent was obtained from each study subjects in the community and also those eligible to participate in the study after screening at the PHC prior to data collection and ocular examination. Subjects requiring specialist ophthalmic consultation were referred for further management at NRS Medical College and Hospital.
Results:
Among 298 subjects attending the ophthalmology clinic of the PHC, most were above 50 yrs of age (47.4%) and were almost equally divided among both genders. Almost one-third of the study population belonged to socioeconomic strata Class IV according to modified Prasad's scale followed by Class III (Table:1).
| Number | % | |
|---|---|---|
| Age group | ||
| 0-9 | 2 | 0.7 |
| 10-19 | 19 | 6.4 |
| 20-29 | 36 | 12.1 |
| 30-39 | 44 | 14.8 |
| 40-49 | 50 | 16.8 |
| 50-59 | 67 | 22.5 |
| 60-69 | 56 | 18.8 |
| 70-80 | 24 | 8.1 |
| Gender | ||
| Female | 150 | 50.3 |
| Male | 148 | 49.7 |
| Socioeconomic status (Modified Prasad scale) | ||
| I | 24 | 8.1 |
| II | 33 | 11.1 |
| III | 95 | 31.9 |
| IV | 110 | 36.9 |
| V | 12 | 4.0 |
The patients were enquired about the risk factors associated with ocular morbidity and it was found that 18.8% were addicted to smoking and majority (76.5%) were overweight or obese. About 42% view television for 2 or more hours per day and use coal, wood or kerosene for cooking. Diseases like Diabetes Mellitus and Hypertension were found to be present in 22.8% and 14% patients respectively. Cataract surgery was already done in one or both eyes in 15.5% patients.(Table:2).
| Risk factors | Number | Percentage |
|---|---|---|
| Addiction | ||
| Alcohol | 18 | 6.0 |
| Smoking | 56 | 18.8 |
| Chewing tobacco | 68 | 22.8 |
| Body mass index | ||
| <18.5 | 4 | 1.3 |
| 18.5-22.9 | 65 | 22.1 |
| 23-25 | 68 | 22.8 |
| 25-30 | 129 | 43 |
| >30 | 32 | 10.7 |
| Average duration of Television viewing per day (in hours) | ||
| 0 | 96 | 32.2 |
| 1 | 75 | 25.5 |
| 2 | 57 | 18.8 |
| 3 | 59 | 20.1 |
| 4 | 5 | 1.3 |
| 5 | 6 | 2 |
| Type of cooking fuel used* | ||
| LPG | 203 | 68.5 |
| Kerosene | 76 | 25.5 |
| Coal /Wood / Cowdung | 51 | 16.7 |
| Family history in 1st degree | ||
| Diabetes mellitus | 38 | 12.8 |
| Hypertension | 24 | 8.1 |
| Cataract | 22 | 7.4 |
| Medical history[1] | ||
| Diabetes mellitus | 68 | 22.8 |
| Hypertension | 42 | 14.1 |
| Cardiovascular diseases | 28 | 9.4 |
| Migraine | 17 | 5.7 |
| Respiratory distress | 7 | 2.3 |
| Cancer | 9 | 3.0 |
| Surgical history* | ||
| Cholecystectomy | 6 | 2 |
| Cataract surgery | 46 | 15.5 |
* Multiple responses
Difficulty with vision was the commonest complain followed by watering, burning and itching sensation, pain and redness. Other symptoms included foreign body sensation, light sensitivity and swelling of eyes. Night blindness was present in 2% cases.(Fig:1)
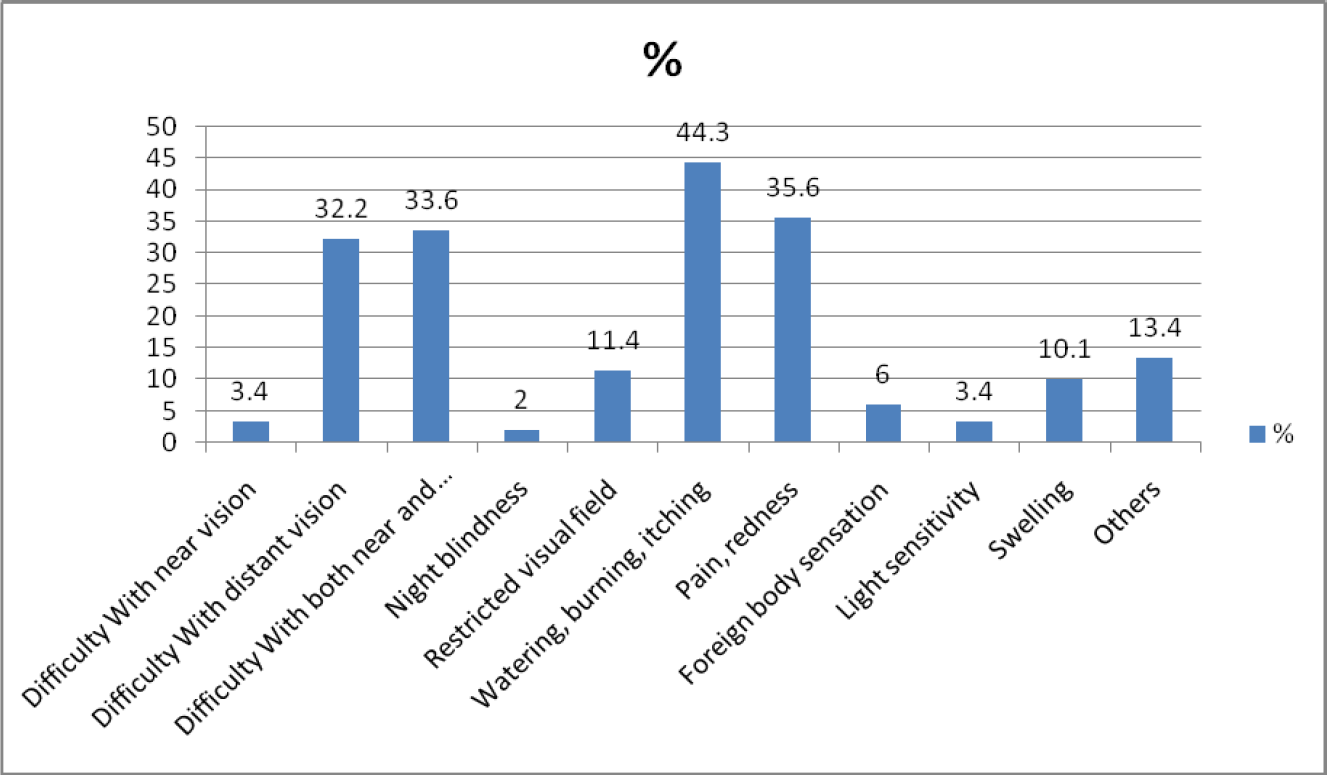
- Distribution of patients according to their presenting complaints (n= 298)
Various ocular morbidities detected during the study are shown in Table:3. After detailed examination it was found that refractive errors (myopia & hypermetropia) were the commonest morbidity among all age groups followed by cataract and allergic conjunctivitis. While cataract was detected mostly among persons greater than 40 years, allergic conjunctivitis was common among younger age group 20 to 39 years.(Fig:2).

- Bar diagram showing distribution of most commonly reported eye conditions according to age group
| Diagnosis of Eye condition | Number | % |
|---|---|---|
| Myopia | 75 | 25.2 |
| Hypermetropia | 5 | 1.7 |
| Amblyopia | 2 | 0.7 |
| Presbyopia | 56 | 18.8 |
| Allergic conjunctivitis | 60 | 20.1 |
| Dry eyes | 9 | 3.0 |
| Chalazion / stye | 28 | 9.4 |
| Glaucoma | 5 | 1.7 |
| Cataract | 70 | 23.5 |
| Pseudophakia | 46 | 15.4 |
| Corneal opacity | 4 | 1.3 |
| Foreign body | 6 | 2.0 |
| Diabetic retinopathy | 2 | 0.7 |
| Iritis | 4 | 1.3 |
| Dacryocystitis | 2 | 0.7 |
| Squint | 4 | 1.3 |
| Traumatic haemorrhage | 2 | 0.7 |
| Others | 8 | 2.7 |
Cataract was found to be significantly associated with diabetes and hypertension (P=0.001) and allergic conjunctivitis was associated significantly with hypertension (P=0.007), depicted in Table:4. About 60% of the patients were treated medically, almost half underwent refractive testing and a quarter was referred to higher facility for further testing and management
| Diseases | Diabetes mellitus | Hyper tension | Cardiovasular disease | |||
|---|---|---|---|---|---|---|
| Yes | No | Yes | No | Yes | No | |
| (n=68) | (n=230) | (n=42) | (n=256) | (n=2 8) | (n=270) | |
| Any Refractive error (n=132) | 30 | 102 | 20 | 112 | 10 | 114 |
| No refractive error (n=166) | 38 | 128 | 22 | 144 | 18 | 156 |
| P value | P=0.97 | P=0.63 | P=0.50 | |||
| Cataract (n=70) | 26 | 44 | 18 | 52 | - | 70 |
| No cataract (n=228) | 42 | 186 | 24 | 204 | 28 | 200 |
| P value | P=0.001* | P=0.001* | ||||
| Allergic conjunctivitis (n=60) | 12 | 48 | 2 | 58 | 6 | 54 |
| No Allergic conjunctivitis (n=238) | 56 | 182 | 40 | 198 | 22 | 216 |
| P value | P=0.56 | P=0.007* | P=0.85 | |||
* P value < 0.05, significant.
Discussion:
The findings of the present study revealed that refractive errors was the most commonly reported ocular morbidity of which majority was myopia . Cataract was the second most common condition among all causes of ocular morbidity.
Age group wise distribution of eye disorders revealed refractive errors were the commonest in age group less than 60 years. Allergic conjunctivitis although a less serious morbidity commonly affected people less than 20 years of age (13.3%). Proportion of cataracts rapidly increased with an increase in age above 40 to 80 years confirming already established findings from other prevalence studies.(8,9)
Refractive errors were most common in age group between 40-60 years closely followed by age group 20-39 years. This shows that refractive errors are becoming a growing problem even before middle age is reached hence efforts should be directed towards earlier detection of refractive errors in the young and middle aged adults through screening. There was no overall gender difference in patients reporting with ocular morbidities. About one fifth of the patients were addicted to smoking and chewing tobacco.
Almost 40% of the study population reported viewing of television for an average of at least 2 hours per day. A study by Beenish M observed that school children watching TV for less than 1 hour had visual acuity of 6/6 in 42.4%, whereas children watching TV for 1-2 hours, 2-3 hours and >3 hours had lower visual acuity.(10)
There is increasing evidence that traditional biofuel use in cooking causes eye irritation and cataract.(11) Although majority of the patients were using LPG as fuel for cooking yet quite a substantial number of them still used coal, wood or cow dung as fuel exposing them to the harmful effects of smoke.
The proportion of eye patients with Obesity, and known Diabetes mellitus and hypertension was quite high. In this study, Diabetes and hypertension was found to be significantly associated with cataract. However in many of those patients Diabetes and hypertension may remain undiagnosed. A general health status screening can be included in eye screening programme in preventing ocular complications which could lead to blindness.(9)
In the present study 15.5% reported pseudophakia while 23.5 % had cataract of which about half had mature cataract necessitating cataract surgery. Thus it becomes essential to conduct routine awareness and screening programmes on preventable blindness in the community.
A study in China found out that two thirds of those with blindness remained in need of sight-restoring surgery, while others with posterior capsule opacification after cataract surgery needed treatment, and refractive errors needing corrections were common.(12)
The proportion of glaucoma in our study was low however it may be an under estimation as no sensitive and specific method was used for confirmation of glaucoma detected in the PHC.
Interestingly quite a high proportion of the patients with visual complaints could be detected and managed at the PHC level itself by medical management (59.1%) and refraction testing (49.7%) thus effectively reducing referral and ultimately the burden on higher health care facility level. The findings of the present study revealed that simple screening for eye disorders and utilization of trained ophthalmic assistants can enable early detection of eye conditions, prompt treatment and early referral.
References:
- www.who.int/blindness/action plan 2014-2019 (accessed )
- 1998 2000 New Delhi
- Global data on Visual impairment in the year 2002. Bull World Health Organ. 2004;82:844-51.
- [Google Scholar]
- Refractive error blindness. Bulletin of the World Health Organization. . 2001;79(3):237-243.
- [Google Scholar]
- Konduru4and Christina Mary P Paul5. Study of uncorrected refractory error, cataract and selected diseases of eye in urban and rural area near Chennai. Tamil Nadu International Journal of Medicine and Public Health. 2012;2(3)
- [CrossRef] [Google Scholar]
- Isawumi1, Mustapha B Hassan1, Esther O Asekun-Olarinmoye2, Patience O Akinwusi3, Wasiu O Adebimpe2, Christopher O Alebiosu3 Prevalence and causes of ocular morbidity seen among rural adult population of Osun State, southwest Nigeria. Ann Trop Med Public Health. 2013;6:465-71.
- [CrossRef] [Google Scholar]
- Effect of television watching on vision of school children in semi urban area of Kashmir. Int J Res Med Sci. 2014;2(2):672-676.
- [CrossRef] [Google Scholar]
- Tears while cooking: an indicator of indoor air pollution and related health effects in developing countries. Environmental Research. 1997;75:12-22.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and outcomes of cataract surgery in rural China the China nine-province survey. Ophthalmology. 2010;117:2120-8.
- [CrossRef] [PubMed] [Google Scholar]




