
Translate this page into:
Involvement of the clinical departments of a medical college in a rural area in the Revised National Tuberculosis Control Programme in India
Address for correspondence: The Editor/ Managing Editor, Journal of Comprehensive Health, Dept of Community medicine, NRS Medical College, 138, AJC Bose Road, Kolkata-700014
Corresponding author: Abhijit Mukherjee, Department of Community Medicine North Bengal Medical College, Sushrutanagar, Darjeeling E-mail: drabhijit71@gmail.com, Phone: 9433187412, 8583930315
Abstract
Introduction:
In addition to their role in the diagnosis and treatment of tuberculosis, medical colleges are involved in imparting knowledge and skills to the future generation of medical doctors. In order that RNTCP runs smoothly, it is important that all clinical departments are involved in RNTCP and manage their TB patients according to their guidelines.
Objectives:
To assess the attendance of TB cases at the clinical departments of a medical college and the categorizing practices of these departments reflecting their involvement in RNTCP.
Materials and methods:
The study was conducted at the NBMC between August and October 2015. Data on patients diagnosed as tuberculosis and categorized as per RNTCP in the clinical departments of the medical college were collected from the office of the MO-TC using pretested schedules and analyzed.
Results:
Of the 230 diagnosed cases, 83 were diagnosed at the chest and 147 at the other non-chest departments. Most of the pulmonary TB cases were diagnosed by the chest department (61.9%) but most of the extra-pulmonary cases were diagnosed by the non-chest departments (82.7%). Most of the cases of tuberculosis, and that were diagnosed at the chest department were categorized and treatment initiated by the same department. In non-chest departments categorization was done in 81.1% of pulmonary and 64.5% of extra-pulmonary cases.
Discussion and Conclusions:
Students at the non-chest departments are not being acquainted with the treatment protocols and categorization principles of RNTCP. Only by actively associating with it, can doctors in the making be encouraged to follow RNTCP in actual practice.
Keywords
RNTCP
Medical College
clinical departments

Introduction:
The medical colleges play an important role in the diagnosis and treatment of tuberculosis. As teaching institutes the MC are also involved in imparting knowledge and skills to the future medical practitioners, that is the internees, house surgeons and post graduate trainees of the different departments and under-graduate students. Teachers at the medical colleges shape the attitudes and prescribing habits of the undergraduate and post graduate students.
The first national consensus conference on TB, held in 1997 at New Delhi emphasized the role of the medical colleges in the Revised National Tuberculosis Control Programme (RNTCP).[1] Since then efforts have been undertaken to involve the medical colleges in RNTCP through sensitization seminars, training for medical college faculty staffs at the Central TB Institutes, and different national and zonal level workshops. The First National Task Force (NTF) meeting for involvement of medical colleges in the RNTCP, 2002, identified seven premier medical colleges in different zones of the country as nodal centres for the RNTCP to take this initiative forward.[2] In 2007 the NTF group work sent recommendations to MCI for inclusion on RNTCP DOTS for the management of TB in UG & PG clinical teaching curricula of all specialties.[3] The Report of the Eighth NTF workshop for enhancing the involvement of MC under RNTCP emphasizes the participation of maximum disciplines in RNTCP. As on 30th October 2009 all of the 30 medical colleges in eastern India have been involved in the formation of core committee, establishment of Designated Microscopy Centre (DMC) and Directly Observed Treatment-Short Course Chemotherapy (DOTS) center in the medical colleges.
In order that the RNTCP runs smoothly in the medical colleges, it is important that all clinical departments, in addition to those departments that run the DOTS centre at the medical colleges, are involved in the programme and manage their TB patients according to the RNTCP guidelines.[4] Also regular exposure of junior doctors to RNTCP will encourage them to follow the programme guidelines during their professional careers within or outside the medical colleges.
The interaction between the academicians of the medical colleges and the programme managers is sparse and on many occasions discordant regarding management of tuberculosis patients.[5] The young doctors in training seldom get an opportunity to practice what is preached to them. As a result, the facilities available under the RNTCP are seldom utilized to the full extent possible. The present study attempts to assess the diagnostic and categorizing and referral practices of the different clinical departments of North Bengal Medical College, Darjeeling, a l medical college in a rural area in the state of West Bengal in India.
Materials and Methods:
This was a retrospective cross-sectional study using medical records and registers. The data was collected on disease characteristics and the categorization practices for all tuberculosis patients diagnosed in the different clinical departments of the North Bengal Medical College between August 2015 and October 2015. Data was collected on pretested schedules and transferred on to the MS Excel (version 97-2003, Microsoft Corp.) and double checked to ensure correctness and completeness. Analysis was carried out using the Epi-Info software (version 2007, CDC, Atlanta).
Results:
A total of 234 patients were diagnosed and treated by the RNTCP during the study period. Four entries were incomplete and were not included in the analysis. All cases were divided into 2 groups i.e. patients diagnosed either at the department of chest medicine or patients diagnosed at the non-chest departments. Of the total; of 230 cases, 83 cases (P = 60, EP = 23) were diagnosed at the chest and 147 cases (P =37, EP =110) diagnosed by the other departments. The median age was 32 (Inter-quartile range 24 - 47) years in patients diagnosed at the chest department and 30 years (Inter-quartile range 20 - 40) in the non-chest departments, while the sex distribution was 3:2 (M:F) in the chest and 2:1(M:F) in the non-chest departments.
The departments that diagnosed a higher number of cases were Chest Medicine (36.1%) and General Medicine (38.2%). The other departments are also involved in the diagnosis of tuberculosis cases although to a much lesser extent. (Figure 1)
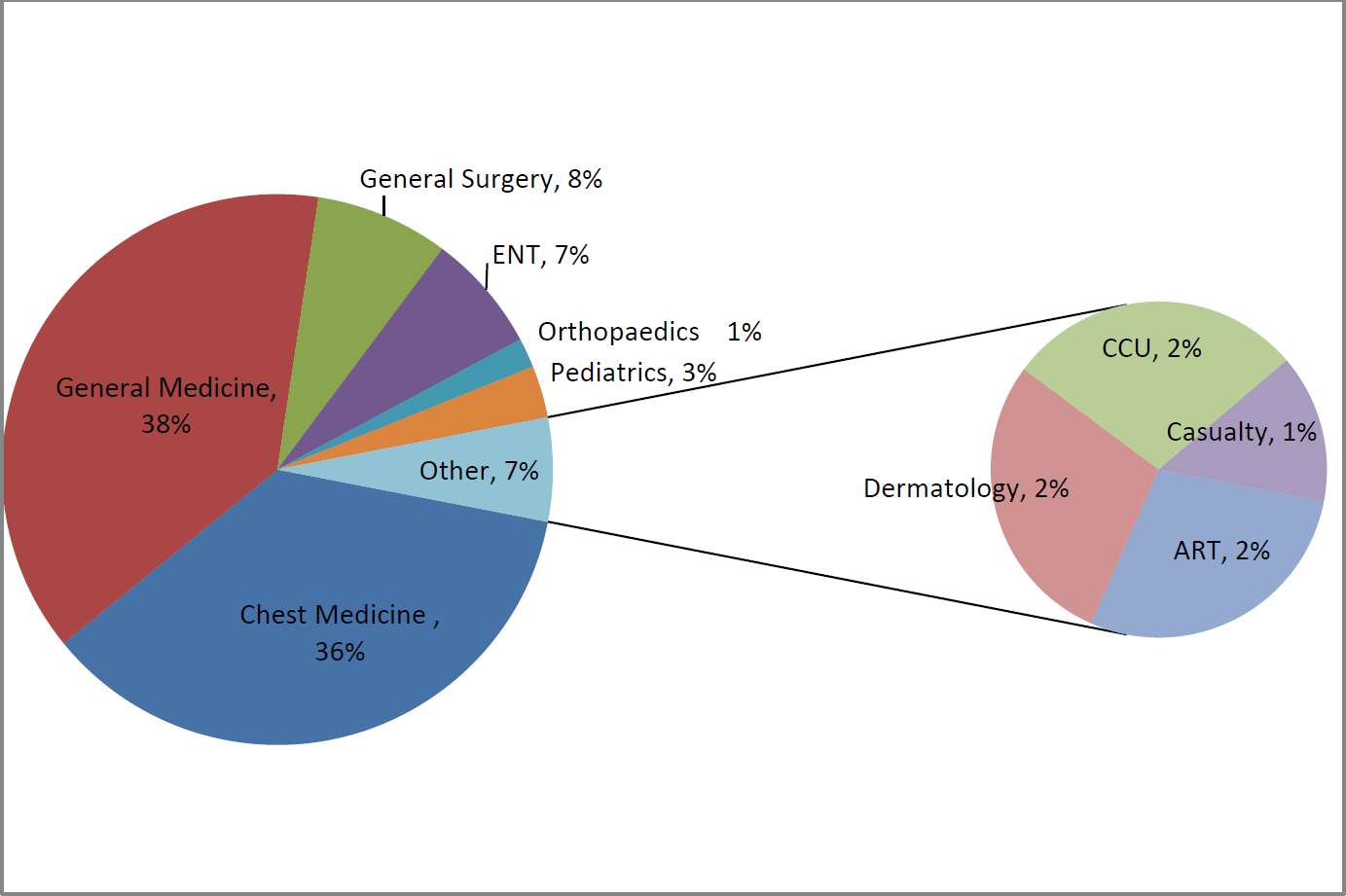
- Department-wise distribution of patients diagnosed as tuberculosis
Most of the pulmonary TB cases were diagnosed by Chest department (61.9%) but most of the EPTB cases were diagnosed by non-chest department (82.7%). Among cases with pulmonary TB most were smear positive (69.1%).
Lymphadenopathy was the commonest among EPTB cases with 52 (39.1%) of the total 133 (type not recorded in two) EPTB cases diagnosed at the medical college. Of them the majorities (42.3%) were cases of cervical lymphadenopathy and diagnosed at the non-chest departments of the medical college. Pleural Effusion and TB meningitis were the second and third most common diagnosis at 21.8% and 13.5% respectively among EPTB cases. Most of these were diagnosed at the non-chest departments. (Table 1)
| Classification | Total | Non-chest departments (%) | Chest Medicine (%) |
|---|---|---|---|
| Pulmonary | 97 | 37(38.1) | 60(61.9) |
| Smear positive | 67 | 27(40.3%) | 40(59.7%) |
| Smear negative | 30 | 10(33.3%) | 20(66.7%) |
| Extrapulm onary | 133 | 110(82.7%) | 23(17.3%) |
| Pleural Effusion | 29 | 22(75.9%) | 7(24.1%) |
| Lymph Node TB | 52 | 41(78.8%) | 11(21.2%) |
| Pericardial Effusion | 1 | 1(100%) | 0 |
| Abdominal TB | 15 | 12(80%) | 3(20%) |
| Musculoskeletal | 12 | 12(100%) | 0 |
| TB Meningitis | 18 | 18(100%) | 0 |
| Skin & soft tissue | 3 | 2(66.7%) | (33.3%) |
| Miliary/ Lung Granuloma | 1 | 1(100%) | 0 |
| EPTB(non-specified) | 2 | 1(50.00%) | 1(50.00%) |
Most of the cases of tuberculosis, and that were diagnosed at the chest department were categorized (Pulmonary =98.3%, EPTB =87%) and treatment initiated by the same department. In Non-Chest Departments categorization done in (Pulmonary =81.1%, EPTB =64.5%) cases. (Table 2)
| Department | Disease type | Not categorized (%) | Categorized (%) |
|---|---|---|---|
| Non Chest Departments | Pulmonary | 7(18.9) | 30(81.1) |
| Extrapulmonary | 39(35.5) | 71(64.5) | |
| Chest Medicine | Pulmonary | 1 (1.7) | 59(98.3) |
| Extrapulmonary | 3(13) | 20(87) |
Discussion:
Following decentralization of the diagnostic facilities under the RNTCP, sputum positive tuberculosis patients are increasingly being diagnosed at the peripheral heath facilities. However, lack of specialist physicians and proper diagnostic facilities in these peripheral centres cause patients with extrapulmonary tuberculosis (EPTB) to be referred to the medical college for diagnosis or confirmation. EPTB cases constitute around 57.83 % of the total TB cases in populations with low HIV prevalence.[6] The significantly higher proportions of EPTB cases diagnosed at the medical college, as seen in the present study, are probably the result of this referral bias. A similar increased incidence of EPTB cases have been documented in unpublished studies from the Tuberculosis Clinic at the All India Institute of Medical Sciences, (AIIMS), New Delhi and the Sri Venkateswara Institute of Medical Sciences (SVIMS), Tirupati, where 53 and 30.4 per cent cases among the total TB cases were EPTB during the period 1994-2002. The involvement of these non-chest departments is therefore critical for the successful running of the programme.
Lymph node tuberculosis and pleural effusions are the commonest forms of extrapulmonary tuberculosis attending any tertiary care hospital. Organ wise EPTB case detection is not strictly limited to the concerned departments. A case of genital tuberculosis may be diagnosed at the medicine, surgery or dermatology departments depending on the preferential attendance of the patient to these departments or the treatment preferences of the attending physicians. So organ wise breakup of tuberculosis does not correspond to the departmental attendance of patients in a medical college. An extensive search of the available literature failed to reveal any information on the contribution of individual departments of a medical college in the total number of tuberculosis cases diagnosed.
Although all departments of the medical college are diagnosing cases of tuberculosis, a section of these patients diagnosed in the non-chest departments are being referred to the chest department for categorization, treatment initiation and follow up. Such referrals to the chest department increase the workload of this department substantially. More importantly, students at the non-chest departments do not get a chance to get acquainted with the treatment protocols and categorization principles of the RNTCP. They will not be conversant with the programme guidelines and will hence be discouraged to practice them once they start treating patients independently.
Only by actively associating with the RNTCP for DOTS implementation [7] can the doctors in the making be encouraged to follow RNTCP in actual practice. Although in principle all the medical colleges have agreed upon it during the national and task forces meetings a thorough analysis reveals that participation of the non chest departments in RNTCP is less than satisfactory.
However, the number of patients in the present study was small and in not reflective of the diagnostic and referral practices of all medical colleges in general. Similar studies need to be done in other medical colleges to assess the involvement of their clinical departments in the RNTCP.
Conclusion:
In order that the RNTCP runs smoothly, it is important that all clinical departments, in addition to the chest department of a medical college are involved and manage their TB patients according to the guidelines laid down by the programme. Only by actively associating with the RNTCP for DOTS implementation can the doctors in the making be encouraged to follow RNTCP in actual practice.
Conflict of interest
The authors have no conflict of interest to declare.
References
- Division, Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India. In: National Consensus Conference on Tuberculosis Control. 1997. Also available at www.tbcindia.org
- [Google Scholar]
- 29th - 31st October, 2002. Available at www.tbcindia.org (accessed )
- 2007. Available at www.tbcindia.org (accessed )
- Are all patients diagnosed with tuberculosis in Indian medical colleges referred to the RNTCP? Int J Tuberc Lung Dis. 2012;16(8):1083-1085.
- [CrossRef] [PubMed] [Google Scholar]
- Managing the Revised National Tuberculosis Control Programme in your area. Central TB Division. In: Directorate General of Health Services. 2005.
- [Google Scholar]
- Is the DOTS strategy sufficient to achieve tuberculosis control in low-and middle income countries? Need for interventions in universities and medical schools. Int J Tuberc Lung Dis. 2003;7:509-15.
- [Google Scholar]




