Translate this page into:
Critical Appraisal of Mass DEC Compliance In A District of West Bengal
Address for correspondence: The Editor/ Managing Editor, Journal of Comprehensive Health Dept of Community medicine NRS Medical College, 138, AJC Bose Road, Kolkata-700014
Corresponding author: Dr. Anima Haldar Flat No B-27/14 ECTP Phase IV Kolkata - 700017 Email Address: anima_h@redifmail.com Mobile No: 0916324262
Abstract
Background & Objectives:
As a part of Revised Filaria control strategy, MDA programme was implemented in Murshidabad district from 29th - 31st December 2008. A cross sectional study was carried out to assess drug compliance after Mass Drug Administration of DEC and the factors responsible for poor compliance among the population of Murshidabad district of West Bengal during Jan 2009. Materials & methods: Total study unit were 120 families covering 3 villages and one municipality ward area (30 families from each area).
Results:
Out of 601 family members, 571 were eligible for Mass drug administration (6 pregnant women and < 2 years age groups (24) were excluded). Drug distribution rate was 91.8%.Overall drug compliance was 42.3%.Total number of defaulters was 330 (57.7%). Non compliance was highest (75.5%) in urban area. Defaulters were more among male than female. Factors responsible for defaulters were no motivation (24.7%), drugs not supplied (22.5%) ,absence at home (13.5%),no faith (10.1%), fear of side effects (10.1%) and others (Forgotten, lack of prior IEC etc), illness, wrong information were 7.8%, 7.3%, 3.9% respectively. Majority has no side effects, only dizziness (3.3%), headache (1.7%), vomiting and others (4.1%) were experienced by the people after consumption of drugs. On an average 40% families were aware about ELF & transmission of disease. Only 43.7% of community members were informed about MDA by Health Workers prior to the implementation of MDA programme.
Keywords
MDA
DEC
ELF
Compliance
IEC
Defaulters

INTRODUCTION
Lymphatic filariasis is a major vector-borne disease problem in many developing countries. About 119million people in 73 countries are infected, 40% in India alone1. The disease is a leading cause of disability2 and impedes socio-economic development of the affected communities3. There are 20 endemic states in India contributing to 95% of the filarial burden in India and it represent 12.8% of the global Wuchereria Bancrofti burden and 20.2% of the Brugia malayi burden.1 In India the National Filaria Control Programme has been in operation since 1955.
Annual single-dose mass treatment with antifilarials -- DEC or ivermectin alongwith Albendazole as co-administration is one of the recommended strategies to achieve the goal of elimination.4
Revised filarial Control Strategy follows the WHO recommendation of annual single dose mass drug therapy with DEC / DEC with Albendazole or Ivermectin with Albendazole is a preventive Chemotherapy adopted by global programme to eliminate Lymphatic Filariasis. Apart from drug efficacy, the other major factor that determines the success of any large scale control / elimination programme is the effective distribution of DEC and good compliance of communities with treatment. The importance of treatment compliance to control programe has recently been highlighted by Plaisier et al5. In pursuit of achieving the goal of elimination of lymphatic filariasis by 2015 Govt. of India has launched nationwide MDA in 202 endemic districts of the country in the year 2004 to have a reported coverage rate of 66.2%6. But actual drug consumption was lower than the reported coverage by peripheral health workers / volunteers. As per the norm, the drug used to be consumed by the eligible population in the presence of drug distributors but on many occasions, the drug was handed over to the family members for consumption later on. It has been observed that a substantial proportion of community members do not consume the drug7.
With the above perspective it is essential to have a post MDA assessment study to determine the status of drug compliance among the beneficiaries and the factors for being defaulters at the consumer level. So the present study was carried out with the objectives of assessing drug (DEC) compliance, the factors responsible for being defaulters, the status of community awareness regarding the transmission of disease (Filariasis), Elimination of Lymphatic Filariasis and Mass Drug Administration Programme, also to suggest some measures for improvement of drug compliance in future.
MATERIALS AND METHODS
MDA Programme was implemented from 29th-- 31st December 2008 in 12 districts of West Bengal, Murshidabad is one of them. Post MDA assessment survey was undertaken during the first week of January 2009 in the district of Murshidabad. The study conducted in three villages-- Ganganarayanpur (Hariharpara block), Beluri (Nabagram block), Baidyanathpur (Burwan block) and one municipality area (ward no—14) of Berhampur Sadar town.
Sampling technique: Stratified Random Cluster Sampling
Sample size: 120 families (30 families from each area).
Selection Process:
1. Three blocks were selected from the district: One block from high coverage area, one block from medium coverage area and another block from low coverage area. 2. Three PHCs were selected, one from each above block randomly.3. From each selected PHC areas one Sub centre area was chosen randomly. 4. Then from each Sub centre area, one village was selected randomly.5. Further, one representative ward in medium coverage town also selected randomly. Thus four clusters (Three villages and one ward) were selected as per guidelines for mid term assessment of mass drug administration8. Each cluster comprises of 30 household or families. So, 30 households were surveyed from each of four clusters. Data were collected through pre-designed and pre-tested schedule by the faculty members of the dept. of community medicine, Calcutta National Medical College to get l5% of the total population as per guidelines supplied. Total l20 families in both rural and urban areas were covered to get at least 600 family members. Finally data for all parameters were analyzed with standard statistical procedure.
OPERATIONAL DEFINITION:
Non compliance - Means did not consume drug in spite of receiving drug,
Defaulter - Means did not consume drug or partially consume drug or those who were not supplied the drug by the drug distributors.
RESULTS
Out of 601 persons surveyed, 571 (95%) were eligible for Mass drug administration. Six pregnant women (1%) and 24 children under 2 years (4%) were excluded from MDA programme. Proportion of both male & female were 50% .
Drug was not distributed to 8.2% of total eligible population by the drug distributors in the district of Murshidabad. In Baidyanathpur village 100% eligible people got DEC but 13%, 12.1% and 7.5% did not receive DEC tablets in beluri, Ganganarayanpur and ward--14 of Berhampur Municipality respectively (Table—I).
| Block / Municipality | Village / Ward | Surveyed population | Eligible population | DEC Distributed No % | Not Distributed No % |
|---|---|---|---|---|---|
| Hariharpara | Ganganarayanpur | 146 | 140 | 123 (87.9) | 17 (12.1) |
| Nabagram | Beluri | 162 | 154 | 134 (87) | 20 (13.) |
| Burwan | Baidyanathpur | 147 | 134 | 134 (100) | |
| Berhampur Municipality | Ward - 14 | 146 | 143 | 133 (92.5) | 10 (7.5) |
| Total | 601 | 571 | 524 (91.8) | 47 (8.2) | |
* Under two years of age group (24) and pregnant women (6) were excluded.
Out of 571 eligible people, 524 (91.8%) received the drug for consumption from the drug distributers. Out of them, only 241(42.3%) persons had consumed full dose and rest (49.5%) consumed either partial dose or had not consumed the drugs at al. Though Ganagnarayanpur belonged to high coverage area (Hariharpara Block) with lowest compliance rate (17.2%) whereas in Baidyanathpur village belonged to low coverage area (Burwan Block) had highest compliance rate of 91.8%.But on the contrary, in urban municipality area (medium coverage area) had highest non-compliance rate (75.5%). (Table-II)
| Block/ Municipality (selected village / ward) | Drug received( n= 524) | Drug Not distributed(n=47) No % |
|
|---|---|---|---|
| Compliance | Non-compliance | ||
| Full dose consumed No % |
Partial / not consumed No % |
||
| Hariharpara (Ganganarayanpur) (n = 140) |
24 (17.2) | 99 (70.7) | 17 (12.1) |
| Nabagram (Beluri) (n =154) |
69 (44.8) | 65 (42.2) | 20 (13) |
| Burwan (Baidyanathpur) (n = 134) |
123 (91.8) | 11 (8.2) | 0 (00) |
| Berhampur | |||
| municipality (Ward No - 14) (n=143) |
25 (17.5) | 105 (75.5) | 10 (7) |
| Total | 241 (42.3%) | 283 (49.5%) | 47 (8.2%) |
DEC was successfully distributed to 91.8% (524/571) of the eligible population (distribution rate) (Figure--I). 42.3% of these compiled with treatment; the remaining 49.5% did not comply, i.e. they received the drug but did not take it. Non-Compliance rate was much higher in Urban Municipality area than Rural area (Table-II).
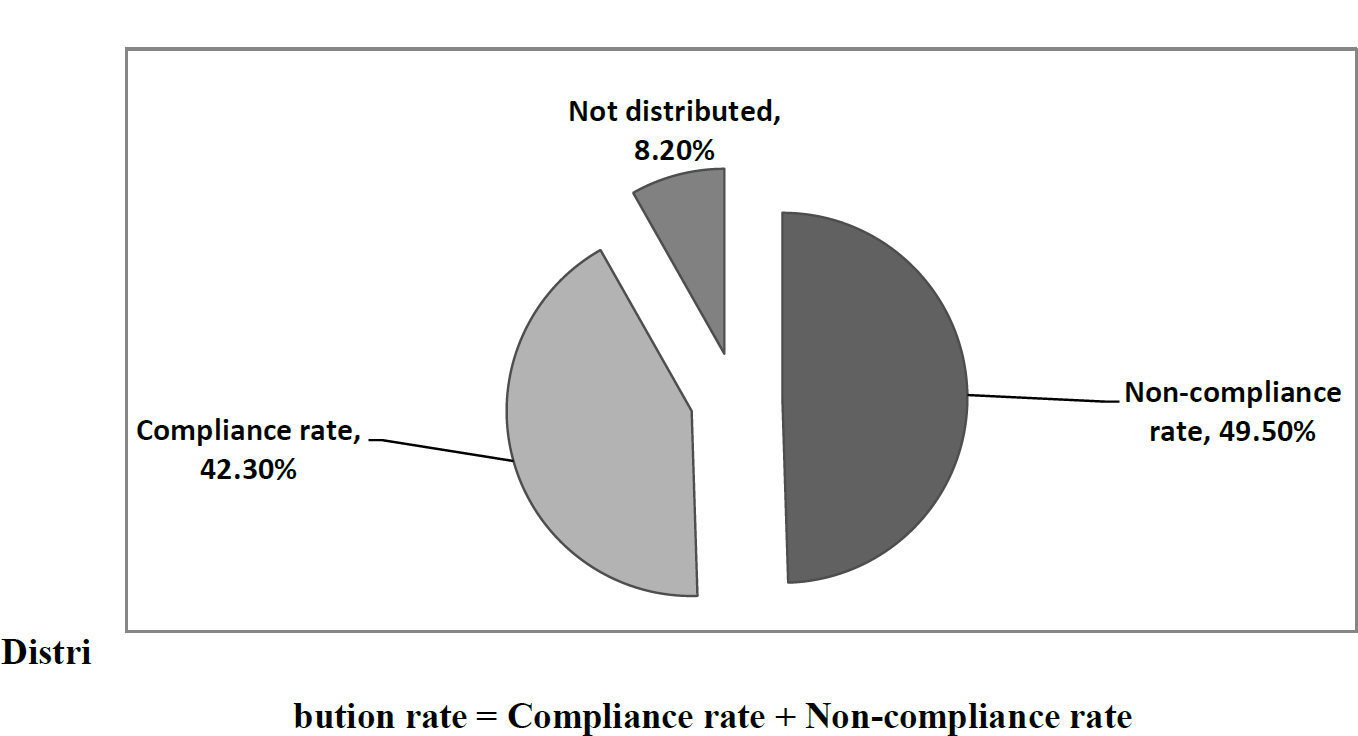
- Overall distribution, compliance and non-compliance rates with DEC treatment
Table III indicated that 330 (57.7%) persons were defaulters which included non compliance population (49.5%) and those whom (8.2%) were not given drugs by drug distributors. Percentage of defaulters was more among males (61.8%) than females (53.7%) in all age groups but the difference was not statistically significant (p > 0.05).
| Age in years | Male Defaulters | Female Defaulters | |||
|---|---|---|---|---|---|
| No | Percentage | No | Percentage | ||
| 2-5 | M (n=16) F (n=20) |
10 | 62.5 | 9 | 45 |
| 6-14 | M (n=70) F (n=55) |
52 | 74.2 | 32 | 58.2 |
| 15+ | M (n=202) F (n=208) |
116 | 57.4 | 111 | 53.3 |
| Total | M (n=288) F(n=283) |
178 | 61.8 | 152 | 53.7 |
P > 0.05
Fig II indicated reasons for not consuming the drugs by the beneficiaries. Highest response was lack of motivation (24.7%) by drug distributors followed by drugs not supplied by distributors (22.5%), then absence at home (13.5%), no faith and fear of side effects each (10.1%), others (forgotten, lack of prior IEC)(7.9%), illness(7.3%) and wrong information (3.9%).
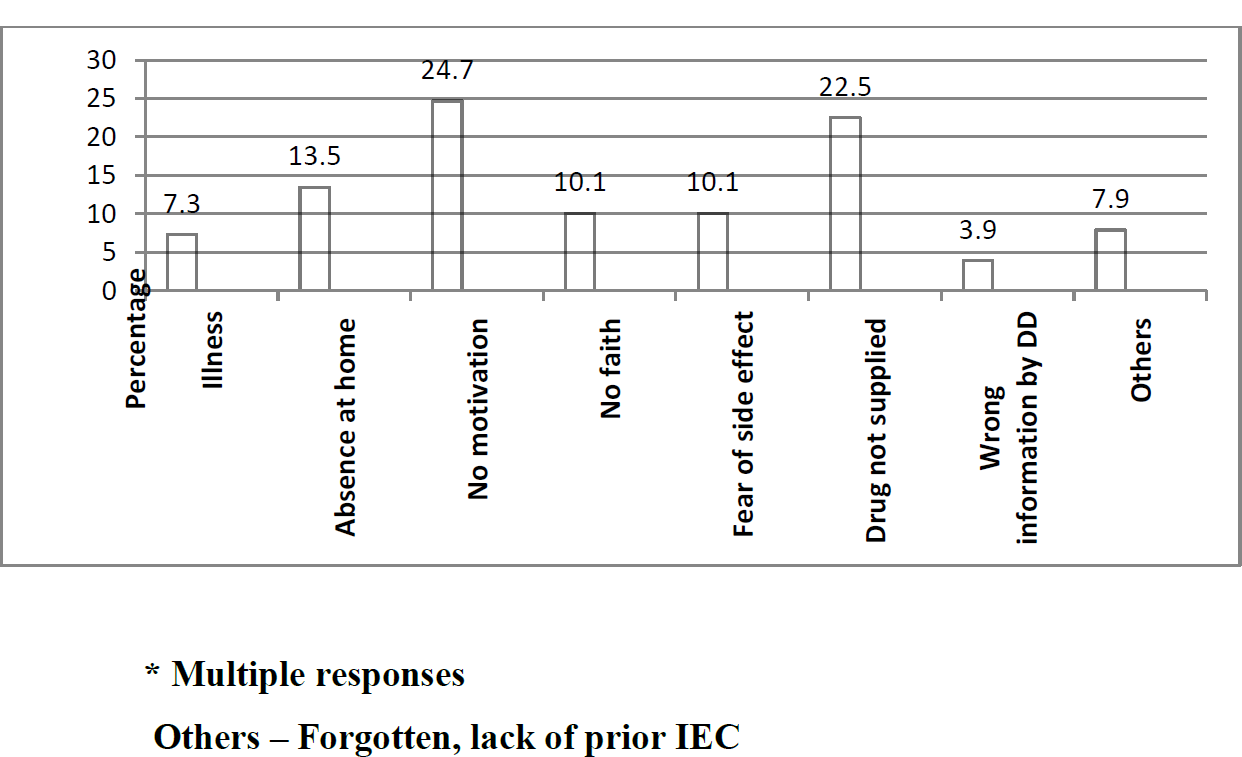
- Reasons for being Defaulters Commented by the Respondent
Regarding side effects Majority (90.9%) had no side effects, only dizziness, headache, vomiting and others were experienced by 3.3%, 1.7% and 4.1% of the consumers respectively. Two cases of Filariasis detected, one in Beluri village of Nabagram block and other one in ward no- 14 of Berhampur Municipality. Only 43.7% of community members were aware about MDA programme, they were informed by the Health Workers. It was also observed from the study that out of total surveyed families, only 53 families (44.1%) were aware regarding ELF and only 45 families (37.5%) were aware about modes of transmission of disease Filariasis.
DISCUSSION
In the present study it was found that overall drug compliance was 42.3% and area specific variation of drug compliance also detected, lowest (17.2%) in high coverage block and highest (91.8%) in rural low coverage area, Compliance higher among females than males in all age groups. These findings corroborated with the findings of earlier study10 where lowest compliance was 52.7% in Purulia (sadar town) Municipality than rural block and compliance rate was also found more among females than males. Regarding side effects, majority of consumers had no side effects only dizziness, headache and vomiting were experienced by 3.3%, 4.1% and 1.7% of the consumers respectively. Similar type of findings also observed by the earlier study8.
The percentage of consumption under supervision in Purulia District of West Bengal in 26th November 2000 was 25.5%, 56.0% in Purulia Municipality and Bandwan Block respctively8 but in the present study nobody got supervised dose indicate that the impetus to programme is gradually decreasing in West Bengal.
In the Present study the DEC distribution rate (91.8%), out of this 42.3% complied with treatment, non-compliance (49.5%) and drug not supplied to 8.2% of the beneficiaries. These findings did not corroborate with the findings of the earlier study9 done at Tamil Nadu by Ramaiah et al where distribution rate was (70%) with 53.5% compliance rate and noncompliance was only 16.5%.
Compliance was more in rural area than urban area and only 5% of the treated population reported side effects observed by the earlier study9,similar observations also found by the present study except reported side effects much higher (9.1%) than earlier one.
However, the severity of side effects caused by DEC is related to mf intensity10 and with expected reduction in mf prevalence11 and intensity12 with each round of treatment, the problem of side effects may subside with progress of the programme.
Annual single dose treatment with DEC is an economical option and provides a good opportunity to undertake an elimination campaign in all endemic states as shown by the Tamil Nadu programme13.
The present study showed that only 43.7% of the community members were informed by Health Workers about MDA programme.
Out of total families, only 53 families (44%) were aware about ELF (elimination of lymphatic filariasis) and 45 families (37.5%) knew regarding modes of transmission of disease. Hence inter-personnel communication and Mass media advocacy both were lacking prior to the implementation of the programme in the district of Murshidabad.
The present study also identified the major factors for being defaulters was no motivation by drug distributors and least by wrong information (side effects). Similar observations also found by the earlier study 14 done at Kerala by Showkath Ali MK et al where poor IEC activities, anti-propaganda, fear of side reaction and lack of adequate prior information were the main reasons for poor compliance. Out of all the surveyed areas, in urban Municipality area the drug distributors did not encourage for consumption of drug, moreover they highlighted on the side effects of drug and not given importance on elimination programme. In Baidyanathpur village of Burwan block, drug distributors were the school children of that locality and with their enthusiastic positive motivation as well as prior awareness of the community resulted in highest drug compliance.
Better public compliance, lower side effects are the benefits of Single dose DEC mass campaign that has eliminated lymphatic filariasis in Japan, Taiwan, South Korea and Solomon Island15.
Some relevant observations found regarding erroneous conception a) towards Drugs distribution i.e. drugs not supplied above the age group 60 years b) towards IEC i.e. NGO volunteers explained the side effects of drugs with a request to attend hospital if it was experienced by consumers. c) supervised dose -- no person found who has taken the supervised dose both in urban and rural areas. It was also observed that no mass communication aids like banners / posters / wall paintings or hoardings were displayed anywhere of the surveyed areas except in the BPHCs.
However, simulation model-based predictions showed that even at a compliance level of 65%--70%, low level transmission and new infections will continue5. Therefore, an urgent need to improve the distribution and compliance in future rounds of DEC mass treatment under the West Bengal programme to consolidate the gains of earlier rounds and achieve elimination of lymphatic filariasis in future.
CONCLUSION
From the present study it can be concluded that the involvement of community volunteers can definitely bring out the desired changes regarding compliance of Mass DEC. Therefore, Health workers as well as community influences / volunteers to be trained for dissemination of knowledge about ELF and transmission of disease along with beneficial effects of Mass Drugs Administration. Prior to further implementation of the programme, area specific IEC campaign to be strengthened. Area specific intervention measures (proper selection drug distributors, adequate training of drug distributors, prior IEC to generate community awareness about transmission of disease and ELF) to be provided in the district of Murshidabad for enhancement of drug compliance in future to achieve the control /elimination of lymphatic filariasis in a reasonable time frame.
ACKNOWLEDGEMENT
The authors were greatful for financial support to the Govt of India & State Govt, department of Health & Family Welfare.Authors also thankful for co-operation & support from State and district officials of Murshidabad District.
References
- Re-assessing the global prevalence and distribution of lymphatic filariasis. Parasitol 1996112:409-28.
- [CrossRef] [PubMed] [Google Scholar]
- Strategies and tools for the control/elimination of lymphatic filariasis. Bulletin of World Health Organisation. 1997;75:491-503.
- [Google Scholar]
- The economic burden of lymphatic filariasis in India. Parasitology Today. 2000;16:251-253.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of Annual Ivermectin treatment for Wuchereria Bancrofti infection. Parasitology Today. 2000;16:298-302.
- [CrossRef] [PubMed] [Google Scholar]
- Mass DEC Campaign for Filariasis in a Hyper-Endemic District of West Bengal, Journal of Communicable Diseases. . 2001;33:192-197.
- [Google Scholar]
- A programme to eliminate lymphatic filariasis in Tamil Nadu state, India: Compliance with annual single-dose DEC mass treatment and some related operational aspects, Trop Med int Health. . 2000;5(12):842-847.
- [CrossRef] [PubMed] [Google Scholar]
- Human Filariasis: A Global Survey of Epidemiology and Control. University of Tokyo press, Tokyo 1976
- [Google Scholar]
- Long term efficacy of single dose mass treatment with diethylcarbamazine citrate against diurnally sub-periodic Wuchereria bancrofti: eight years experience in Samoa. Bulletin of the World Health Organization. 1992;70:769-776.
- [Google Scholar]
- Efficacy of bi-annual administration of DEC in the control of bancroftian filariasis. Journal of Communicable Diseases. 1992;24:87-91.
- [Google Scholar]
- Cost of annual mass single-dose DEC distribution for the large scale control of lymphatic filariasis in Cuddalore district,India. Indian Journal of Medical Research. 2000;110:81-89.
- [Google Scholar]
- Study on the factors affecting the MDA programme in Kerala state. Journal of Communicable Diseases. 2007;39(1):51-6.
- [Google Scholar]
- Recent Advances in Filaria management. Directorate of National malaria Eradication Programme, Ministry of Health and Family Welfare, New Delhi. 1998
- [Google Scholar]




