
Translate this page into:
Cholera outbreak in Kamarhati municipality of West Bengal: Secondary data analysis of a rapid epidemic response
CITATION: Ray S, Mukherjee T, Das A, Chattopadhyay B, Mukhopadhyay DK, Misra R. Cholera outbreak in Kamarhati municipality of West Bengal: Secondary data analysis of a rapid epidemic response. J Comp Health. 2021;9(2):69-74.
CORRESPONDING AUTHOR: Dr Tanmoy Mukherjee, Demonstrator, Department of Community Medicine, College of Medicine and Sagore Dutta Hospital, Kamarhati, Kolkata - 700058 E Mail ID: mukherieetanmov1234@gmail.com
-
Received: ,
Accepted: ,
Abstract
Introduction:
In September, 2021, an outbreak of acute diarrhoeal disease affected different wards of Kamarhati municipality of West Bengal. An epidemic investigation was conducted with the objective of identifying the time, place and person distribution of the epidemic.
Methods:
In this institution based cross-sectional study, an epidemic response team of College of Medicine and Sagore Dutta Hospital (CoMSDH) visited the patients admitted in the infectious diseases ward of the institute and enquired them using a pre-designed proforma. Stools samples were collected and sent for analysis to National Institute of Cholera and Enteric Diseases (NICED), West Bengal. The team also visited the affected wards and collected water samples for laboratory investigations. Collected data were collated in Google sheets and requisite analyses were done in Google sheet, online spreadsheet software. Spatial distributions of cases were shown using QGIS v2.38.
Results:
208 patients admitted in infectious diseases ward of CoMSDH, Kamarhati, Kolkata in between 2nd - 13th September, 2021 were interviewed. The epidemic curve showed a rapid rise on 07th September, 2021 (57 cases) followed by a gradual fall over next 5 days. Majority of cases were clustered in Ward 1,2 and 3 of Kamarhati municipality. The attack rate was highest among the geriatric age group (>60 years) followed by 19-60 years age group. Abdominal Pain (35.71%) and vomiting (28.57%) were commonly associated symptoms. Majority of the respondents (172, 87.76%) used intermittent tap water supply from local municipalities, followed by purchased mineral water (20, 10.20%) and water from Tala tank (4, 2.04%) for their drinking purpose. Stool and water samples revealed the presence of Vibrio Cholerae, O139 ogawa serotype.
Conclusion:
On the basis of the interim analysis, health education was initiated on the domestic treatment of water by boiling or using chlorine solution. Additionally, steps were taken for water treatment at the water treatment plants. This assisted in controlling the outbreak.
Keywords
Vibrio Cholerae O139
Disease Outbreaks
Diarrhoea
QGIS
West Bengal

INTRODUCTION
Acute diarrhoeal disease (ADD) is still considered as a public health concern in India.(1) Various factors like poor socio-economic conditions, inadequate access to adequate sanitation plays an important role in this water borne disease. Approximately 2 billion cases of ADD occur every year globally.(2) ADD is the second leading cause of mortality among under-five children across the world.(2) According to National health profile of India, 116,73,018 cases of acute diarrhoea were reported in 2015.(3,4)
Depending on the causative organism, ADD might be associated with complaints of abdominal pain and vomiting. If left untreated, ADD might lead to fatal outcome, mostly due to dehydration caused by the water loss. Even if not fatal, the water loss might be associated with metabolic acidosis due to dehydration, renal failure and circulatory shock.(2)
Among the various organisms responsible for ADD, Vibrio Cholerae, Bacillus Cereus, Escherichia Coli etc. are most commonly associated in the gangetic West Bengal. ADD tends to occur as a result of contamination of food or water with the causative organism. This might take place due to poor personal hygiene, unsafe environmental condition, lack of adequate safe and wholesome water supply.(2) In the night of 08th September, 2021, College of Medicine and Sagore Dutta Hospital (CoMSDH) were inundated with cases of ADD. Sudden inundation of cases produced a burden on the existing resources of CoMSDH. Department of Community Medicine was entrusted to conduct a rapid investigation of the outbreak. A team was mobilised in the morning of the 09th September, 2021. The team investigated the outbreak with the objectives of identification of the agent (causative organism) and it's time, place and person distribution. In this publication, we present the initial investigation findings of the diarrhoeal outbreak which affected the municipality in the month of September, 2021.
MATERIAL & METHODS
This was an institute based survey with cross-sectional design, conducted in the CoMSDH of Kamarhati municipality. Kamarhati municipality is part of the Barrackpore Sub-division, North 24 Parganas district and surrounded by Baranagar and Panihati municipality. It has 35 wards and a population of 330,211 as per 2011 census.(5) The team visited all the patients who were admitted in CoMSDH with ADD between 2nd September to 13th September, 2021. For this rapid investigation, case definition of ADD was decided as individuals having watery stool in 48 hours prior to admission. Complete enumerations of all admitted cases were done. Considering the admitted patients as respondent, diarrhoeal status of their family members were also enquired for calculation of secondary attack rate.
Data were collected by interviewing the respondents with a pre-designed interview schedule to find out various epidemiologic features on ADD. Emphasis was given on their address (name of the road, ward number) for preparing a chloropleth of affected wards. Date of appearance of watery stool was also enquired along with other presenting symptoms. The latter part was enquired through an open ended question. Information on total family members and number of affected family members was collected for calculation of attack rate. History about attending any gathering/festivity or consuming any "Prasad” in last 3-4 days were enquired for ruling out food borne point source exposure. Source of their drinking water were enquired for ruling out water borne pathogens. Along with the admitted patients, the epidemic investigation team also visited the most affected wards of Kamarhati municipality for an environmental investigation.
In this study, we have collated all data collected by the investigators, report of the stool samples admitted in CoMSDH and report of the water samples collected from the affected wards. A Google Form was created for digitising the data collected in paper form. The collected data were linked to a Google Sheet, an online, free of cost, spreadsheet programme. The required analysis was done in Google Sheet. The data were expressed in tables and graphs. Qualitative data were expressed in frequency and percentages. The chloropleth map was created using QGIS.(6-8) The study has received institutional ethical clearance from the Institutional Ethics Committee of CoMSDH (letter number CMSDH/IEC/252/09-2021 dated 25th September, 2021).
RESULTS
208 patients admitted in infectious diseases ward of CoMSDH, Kamarhati, Kolkata in between 2nd - 13th September, 2021 were interviewed. Among the admitted patients 12 individuals refused to share information, in spite of counselling them about the importance of the investigation. So, response rate was 94.23%. It was found that Maximum number of cases(57) had onset of symptoms on 07th September, 2021 (Figure 1). The epidemic curve showed a rapid rise on 07th September, 2021 followed by a gradual fall over next 5 days. Majority of cases were clustered in Ward 1,2 and 3 of Kamarhati municipality, highest being Kamarhati ward no. 3, followed by ward no. 1 and 2 (Table 1). Some(29) patients could not mention their ward number. However, it was unlikely to change the distribution of the affected ward. On interviewing the admitted patients about their family members it was found that the attack rate was highest among the geriatric age group (≥60 years) followed by 19-60 years age group (Table 2). Majority of the affected person were female (104, 53.06%). Out of 196 respondents abdominal Pain (35.71%) and vomiting (28.57%) were commonly associated symptoms. Majority of the respondents (172, 87.76%) used intermittent tap water supply from local municipalities, followed by purchased mineral water (20, 10.20%) and water from Tala tank (4, 2.04%) for their drinking purpose. Only 5 (2.55%) respondents had festive get together. Presence of O139 serotype ogawa biotype of Vibrio Cholerae was found in the stool swabs and water sample from the affected area.
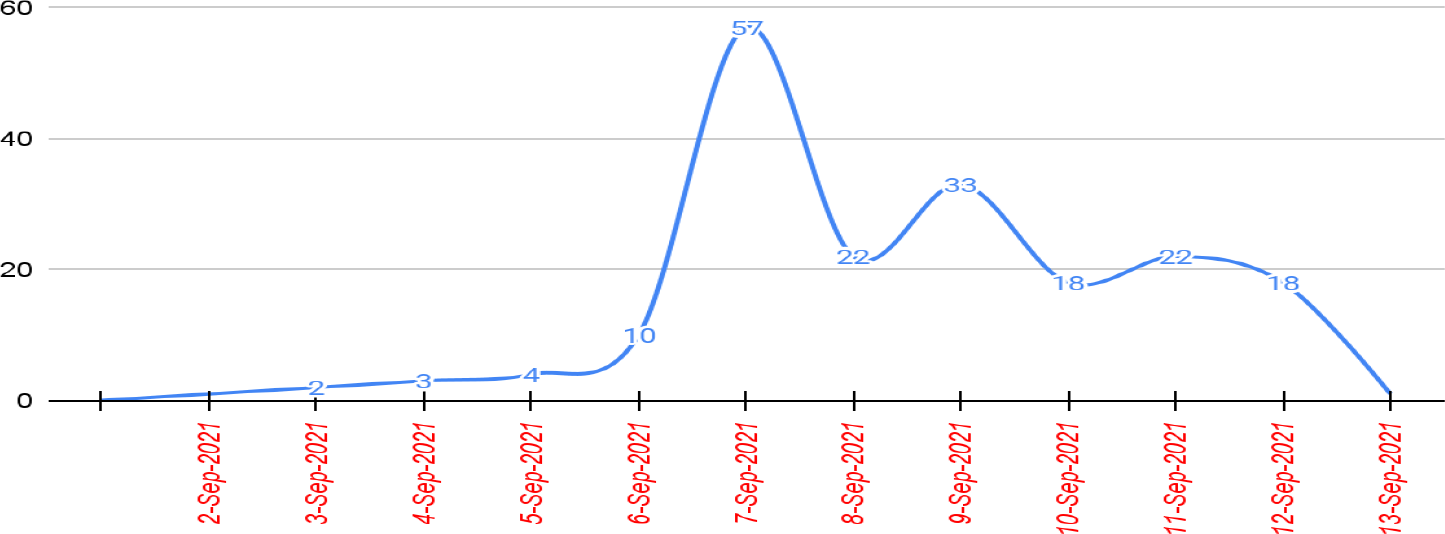
- DISTRIBUTION OF DIARRHOEAL CASES ADMITTED IN COMSDH ACCORDING TO THEIR TIME OF APPEARANCE OF SYMPTOMS (N=196)

- CHOLROPLETH DEPICTING THE DISTRIBUTION OF ADMITTED DIARRHOEAL CASES OF KAMARHATI MUNICIPALITY IN COMSDH ACCORDING TO THEIR WARD NUMBER (N=160#)
| Ward Number | Frequency | Percentage |
|---|---|---|
| Kamarhati Municipality | ||
| 1 | 36 | 18.65 |
| 2 | 21 | 10.88 |
| 3 | 49 | 25.39 |
| 4 | 6 | 3.11 |
| 5 | 6 | 3.11 |
| 6 | 7 | 3.63 |
| 7 | 8 | 4.15 |
| 8 | 6 | 3.11 |
| 10 | 1 | 0.52 |
| 11 | 1 | 0.52 |
| 12 | 2 | 1.04 |
| 13 | 1 | 0.52 |
| 14 | 1 | 0.52 |
| 19 | 1 | 0.52 |
| 20 | 1 | 0.52 |
| 23 | 1 | 0.52 |
| 26 | 2 | 1.04 |
| 27 | 1 | 0.52 |
| 28 | 2 | 1.04 |
| 29 | 1 | 0.52 |
| 32 | 1 | 0.52 |
| 33 | 1 | 0.52 |
| 34 | 1 | 0.52 |
| Ward number Not Known | 29 | 15.03 |
| Panihati Municipality | ||
| 4 | 1 | 0.52 |
| 6 | 1 | 0.52 |
| 10 | 2 | 1.04 |
| North Dumdum Municipality | ||
| 4 | 1 | 0.52 |
| 30 | 1 | 0.52 |
| Khardah Municipality | ||
| 17 | 1 | 0.52 |
| Age group | Population | Cases | Attack Rate (%) | ||
|---|---|---|---|---|---|
| Female | Male | Female | Male | ||
| <1 year | 6 | 1 | 0 | 0 | 0 |
| 1-4 years | 21 | 10 | 1 | 1 | 6.45 |
| 5-18 years | 94 | 108 | 7 | 11 | 8.91 |
| 19-60 years | 279 | 286 | 62 | 48 | 19.47 |
| >60 years | 27 | 28 | 5 | 6 | 20 |
DISCUSSION
Laboratory and environmental evidence indicated that the ADD outbreak was due to Vibrio Cholerae contamination of the domestic water supply, occurred at the water pumping station for ward 2 and 3. Presence of watery stool along with abdominal pain and vomiting indicated involvement of small intestine. Relative absence of fever, bloody stools and no history of food intake in festivals in majority of cases helped to rule out Escherichia Coli, Bacillus cereus, Salmonella, Campylobacter, Listeria.(9,10) Acute nature of the cases ruled out presence of Giadia.(9,10) Epidemiologically, thus, involvement of Vibrio Cholerae was suspected. This hypothesis was later corroborated by the laboratory investigation result of stool and water samples. Stool swabs collected from the patients and water samples collected from the most affected Wards showed presence of Vibrio Cholerae.
The contamination might be related to the massive rain which had taken place in this part of West Bengal, between 25th August to 05th September, 2021. This environmental phenomenon led to backflow of river water from the Ganges in the living areas. Presence of Vibrio Cholerae in the gangetic water is a well known fact.(11) Earlier studies have shown presence of Vibrio Cholerae, ogawa biotype in the gangetic water.(11,12) In our study, laboratory investigation confirmed the presence of O139 serotype ogawa biotype of Vibrio Cholerae in the stool sample of the affected individuals along with the water sample collected from the municipal tap water supply in ward 2 and 3 and from water pumping station. Worsening of primitive waste disposal methods along with water stagnation due to heavy rain and poor monitoring of quality check at water treatment plant probably acted together leading to this outbreak. Effective surveillance and response system for the water treatment and supply is essential for combating different water borne diseases.
Laboratory investigation further revealed that the organism was sensitive to Doxycycline and Azithromycin and resistant to other commonly used antibiotic like Ampicillin, Nalidixic acid, Trimethoprim-Sulfamethoxazole and Gentamicin. This information, although helpful in controlling the present outbreak, is a matter of concern in the medium to long term. Compared to earlier study by Sur et al in 2002, resistance has developed against nalidixic acid and trimethoprim-sulfamethoxazole combination.(12)
Almost 9 out of the 10 admitted person used intermittent tap water supply from Kamarhati Municipality. Although, in absence of information about proportion of population using different water sources, this information could not be generalised to comment upon contamination of the municipality supplied water. However, presence of Vibrio Cholerae in the water pumping station for ward number 2 & 3 provided indirect support to the contaminated water hypothesis. Interestingly, the attack rate was very less among the under five compared to adults. This information is in accordance with findings from different global studies from Zimbabwe to Nigeria.(13,14) However, earlier studies in West Bengal and Assam used to report higher attack rate among younger age group.(12,15,16) Our difference in study finding from earlier studies in West Bengal might be attributed to temporal difference of 30 years. Additionally, it is possible that children were given water after treating them domestically (eg, boiling water). However, this information was not enquired at the time of data collection.
The epidemic team, during their visit on 10th September, 2021 to Kamarhati municipality, urge them to increase the health education activities among the affected population. General population were advised to use water after boiling or treating with chlorine solution at household level. Active surveillance for early case detection and management was also strengthened. Water treatment plants were instructed to optimise the residual chlorine content in water. Prompt and emergency action taken on the basis of this survey reported helped to control the outbreak by 13th Septem ber, 2021. One of the limitations of this survey was that it collected information only from the hospitalised patients. It is thus possible that cases in the other wards might have been missed and a false high representation of cases from Ward 1,2 and 3 were presented with. However, presence of Vibrio Cholerae in the water pumping station of Ward 2 & 3 indicated that this false high representation, even if happened, did not alter the survey finding significantly. Higher number of cases in ward number 1 might be due to the fact that Craig lane, the most commonly affected road, was the boundary of ward number 1 & 3. Despite this limitation, the study provided useful information to stakeholders on actions that will likely to be helpful in avoiding future such outbreaks; e.g., provisioning of safe and wholesome water to the community members, continuous monitoring and surveillance of water quality at water pumping station and at randomly selected municipality taps, strengthening of reporting of cases with fever, diarrhoeaetc from the community by Honorary Health Workers in municipality areas. On the basis of the interim analysis, health education was initiated on the domestic treatment of water by boiling or using chlorine solution. This assisted in controlling the outbreak and proved the importance of health education in controlling different outbreaks once again.
AUTHORS CONTRIBUTION
All the authors have read through the final manuscripts and transferred the rights to the corresponding author to make necessary changes as per the request of the journal, do the rest of the correspondence on their behalf.
REFERENCES
- Socio-demographic and environmental factors associated with diarrhoeal disease among children under five in India. BMC Public Health. 2020;20(1):1-11.
- [CrossRef] [PubMed] [Google Scholar]
- Diarrhoeal disease [Internet] Available from: https://www.who.int/news-room/fact- sheets/detail/diarrhoeal-disease (accessed )
- [Google Scholar]
- Investigation of acute diarrhoea outbreak at Narasapura, Kolar. Int J Community Med Public Health. 2019;6(7):3029-32.
- [CrossRef] [Google Scholar]
- Prevalence of Intestinal Parasitosis among Under-Five Children in a Rural Community of PurbaBardhaman District, West Bengal. Indian J Community Med Off Publ Indian Assoc Prev Soc Med. 2020;45(4):425-8.
- [CrossRef] [PubMed] [Google Scholar]
- Office of the Registrar General & Census Commissioner, India [Internet] Available from: https://censusindia.gov.in/2011-common/censusdata2011.html (accessed )
- [Google Scholar]
- QGIS Geographic Information System. Open Source Geospatial Foundation, 2009. Open Source Geospatial Foundation Available from: http://qgis.osgeo.org. (accessed )
- [Google Scholar]
- Free Online Surveys for Personal Use [Internet] Available from: https://www.google.com/forms/about/ (accessed )
- [Google Scholar]
- Free Online Spreadsheets for Personal Use [Internet] Available from: https://www.google.co.in/sheets/about/ (accessed )
- [Google Scholar]
- Environmental Vibrio cholerae non O1/non O139 from the Gangetic delta: a diarrhoeal disease purview. International journal of environmental health research. 2017;27(4):241-51.
- [CrossRef] [PubMed] [Google Scholar]
- A localised outbreak of Vibrio cholerae O139 in Kolkata, West Bengal. Indian J Med Res 2002 Apr 115:149-52.
- [Google Scholar]
- Descriptive epidemiology of cholera outbreak in Nigeria, January-November, 2018: implications for the global roadmap strategy. BMC Public Health. 2019;19(1):1-11.
- [CrossRef] [PubMed] [Google Scholar]
- Low case fatality during 2017 cholera outbreak in Borno State, North Eastern Nigeria. Ann Afr Med. 2018;17(4):203.
- [CrossRef] [PubMed] [Google Scholar]
- An Outbreak of Cholera Associated with an Unprotected Well in Parbatia, Orissa, Eastern India. J Health PopulNutr. 2009;27(5):646-51.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Vibrio cholerae O1 serogroup in Assam, India: A hospital-based study. Indian J Med Res. 2017;146(3):401-8.
- [Google Scholar]




