
Translate this page into:
An Assessment of Knowledge, Attitude and Practice about Biomedical Waste Management among Health Care Workers in Primary Health Care Facilities in a District of West Bengal
CORRESPONDING AUTHOR: Prof Sarmila Mallik, C/5, Ideal Association, VIP Road, Kolkata- 700054, West Bengal, India E Mail ID: sarmila46@gmail.com
-
Received: ,
Accepted: ,
CITATION: Dey S, Ghosh R, Mondal S, Mallik S. An Assessment of Knowledge, Attitude and Practice about Biomedical Waste Management among Health Care Workers in Primary Health Care Facilities in a District of West Bengal. J Comp Health. 2022;10(2):72-79. Doi: https://doi.org/10.53553/JCH.v10i02.005
Abstract
Background:
Biomedical waste become hazardous if it is not segregated, treated and disposed properly and poses a serious health problem to health care workers as well as to the community.
Objectives:
To assess the knowledge, attitude and practice about biomedical waste management among the health care workers posted in primary health care facilities in a district of West Bengal.
Methods:
This cross-sectional study was conducted in subcentres, bedded and non bedded primary health centres (PHC) selected by multi stage random sampling. Thus six PHCs and 14 subcenres were chosen. Study population included doctors, nurses, pharmacists, lab technicians, health supervisors, Auxiliary Nurse Midwives and housekeeping staff. Study techniques included interview of the study participants and practice of was observed by an observation check list.
Results:
Knowledge and attitude of the study participants were satisfactory about biomedical waste management, but practice was seen to be very poor. Nurses were seen to be more knowledgeable than other categories of staff. Training and vaccination status were poor. The median knowledge, attitude and practice score had no significant association with age or years of experience of the study participants.
Conclusion:
Repeated training and sensitization workshops should be organized for increasing knowledge and attitude of the health care workers and repeated monitoring is required to improve practice. All the HCWs should be vaccinated properly with Hepatitis B vaccination and tetanus toxoid.
Keywords
Attitude
Gap analysis
Health care workers
Knowledge
Practice
Primary health care facilities

INTRODUCTION
Improper Biomedical Waste Management (BMWM) poses serious public Health problem worldwide. Approximately, 5.2 million people, including children, die every year due to waste-related diseases.1 Biomedical waste (BMW) carries higher risk of infection and injuries than other types of waste increasing the chances of acquiring HBV, HCV and HIV.2 The direct and indirect consequences of improper BMWM includes intentional reuse of disposable materials, air pollution, and production of toxic emissions due to inadequate burning of medical waste, which lead to significant impacts on the environment.3,4
BMW become hazardous if it is not segregated, treated and disposed properly. In addition, the disposal methods impact directly the healthcare workers and on their community.4 In India the risk is higher as proper waste segregation and waste disposal methods either does not exist or not practiced. Many Indian newspapers and magazines have reported that re-use of disposable syringes, needles, catheters, bags, drug vials, bottles, and intravenous drip sets are picked up by rag pickers and purchased by duplicators, recycled, replaced without proper treatment.5
There is an increased global awareness among health professionals about the hazards and also appropriate management techniques but the level of awareness in India is found to be unsatisfactory.6,7 Adequate knowledge about the health hazard of hospital waste, proper technique and methods of handling the waste, understanding of segregation and practice of safety measures can go a long way toward the safe disposal of hazardous hospital waste and protect the community from various adverse effects of the hazardous waste.8
Knowledge, attitude and practice of the health care workers were assessed in several studies conducted predominantly in tertiary care setting, but scarce in primary health care level all over the world. Under this context, the present study was conducted with the objectives to assess the knowledge, attitude and practice of Bio-medical waste management among the health care personnel posted at primary health care facilities of a district of West Bengal and to find out the gaps in BMW management of the selected health facilities.
MATERIAL & METHODS
This descriptive, observational, facility based study with cross sectional design was conducted in primary health care facilities in Murshidabad district of West Bengal, India. Primary health care facilities included subcentres (SC), bedded and non bedded primary health centres (PHC). Study period was January to June 2020.
A multistage random sampling technique was employed in this study. In the first step, two subdivisions of Murshidabad District were chosen randomly out of five sub-divisions considering the feasibility of survey and time constraints. In the second step, considering the PHCs as the sampling unit, in each subdivision 20% of PHCs were chosen by systematic random sampling method. Thus three (3) PHCS each from two subdivisions were selected giving a total of 6 PHCs. Then in the last step form these 6 PHCs 10% Sub. Centers (S.C) had been selected randomly thus giving a total of 14 SCs (total no of S.Cs were 140 and its 10% had been chosen).
Study population were health workers working at SC level viz 2 ANMs and Health supervisors; health care personal of bedded or non-bedded PHCs like -Doctors, Nurses, Pharmacist, Lab. Technician, Housekeeping staffs etc. The health care personnel who are working for at least 3 years in selected health facilities, heard at least the term BMW and had given consent were included in the study. The persons who were not present at the day of visit were excluded from the study.
Independent variables for the study were age, gender, post, working experience of the study participants. Dependent variables were knowledge, attitude and practice of the health care personal about the different aspects of BMWM. Knowledge was assessed by the variables like colour coding of the bags, health hazards, steps of BMWM, segregations, disposal of different categories of waste, sterilization and treatment of the BMW. Attitude towards the BMWM included the importance of disinfection of hospital waste, necessity of BMW rule, importance of team work, issue of segregation, health hazards and perception of BMWM as an extra burden to health workers. Practice for the management of BMW included process of sterilization, use of disinfectant solution, use of personal protective measures, status of immunization, periodic health check up of HCWs and the training received.
A pilot-tested, pre-designed, semi-structured questionnaire having 34 items was prepared in English and then translated to local vernacular (Bengali) by a linguistic expert keeping semantic equivalence. To check the translation, it was re-translated into English by two independent researchers who were unaware of the first English version. Face and content validity of each item/domain had been checked in the presence of public health experts. Reliability was checked by test-retest method (r=0.9).
Study techniques included interview of the study participants and practice of was observed by an observation check list.
To ensure the quality of data, all filled questionnaires were checked for completeness. Data thus collected had been analyzed subsequently in MS Excel and also in STATA 16.0 version.
Informed consent was obtained from the health care personal who were willing to participate in the study. Ethical approval was obtained from the Institutional Ethics Committee, Institute of Public Health Kalyani (IPHK) before commencement of the study.
RESULTS
Table 1 depicted the basic profile of HCWs of studied primary health care facilities. Most of the health care staff belonged to the age of 31-44 years (48.6%) and were females (58.6%). So far as working years were concerned, majority of heath care personnel (48.6%) were working in the same post for <=10 years.
| Characteristics | No | % |
|---|---|---|
| Age (years) | ||
| ≤ 30 | 10 | 14.3 |
| 31 - 44 | 34 | 48.6 |
| ≥ 45 | 26 | 37.1 |
| Gender | ||
| Male | 29 | 41.4 |
| Female | 41 | 58.6 |
| Professional category | ||
| Doctors | 11 | 15.7 |
| Nursing staff (NS) | 10 | 14.3 |
| Pharmacist (PH) | 5 | 7.1 |
| Lab technicians (LT) | 6 | 8.6 |
| Housekeeping staff | 8 | 11.4 |
| Health supervisors | 3 | 4.3 |
| Auxiliary nurse midwife (ANM) | 27 | 38.6 |
| Years of service | ||
| ≤ 10 | 34 | 48.6 |
| 11 - 19 | 13 | 18.6 |
| ≥ 20 | 23 | 32.8 |
Knowledge of health care workers about BMWM
While assessing knowledge it was revealed from Table 2, only one fourth of the health care workers had correct knowledge i.e could utter all the types of BMW and 68.5% could identify the hazardous and non hazardous waste. Here 80% of the nursing staff and 45% doctors had correct knowledge. While assessing colour coding, only 67% could tell all the coloured bags (correct knowledge), out of which 100% of nursing staff had correct knowledge. About the hazards of BMW, only 38% of HCW could tell all the hazards like HIV, Hepatitis B and injuries, where more than half of the doctors didn't have the correct knowledge.
| Correct knowledge | Category of HCW | |||||
|---|---|---|---|---|---|---|
| Doctor (n=11) No (%) | N.S(n=10) No (%) | ph + lt (n=11) No (%) | h.s+anm (n=30) No (%) | Housekeeping staff (n=8) No (%) | Total (n=70) No(%) | |
| Types of BMW | 5(45.5) | 8 (80) | 0 | 4 (13.3) | 1 (12.5) | 18 (25.7) |
| Colour coding | 9 (81.8) | 10(100) | 4(36.4) | 23 (76.7) | 1(12.5) | 47 (67.1) |
| Health hazards | 5 (45.5) | 8 (80) | 3 (27.3) | 11 (36.7) | 0 | 27 (38.6) |
| Steps of BMWM | 5 (45.5) | 8 (80) | 0 | 4 (13.3) | 1 (12.5) | 18 (25.7) |
| Segregation | 11 (100) | 10 (100) | 2 (1.2) | 20 (66.7) | 0 | 43 (61.4) |
| Disposal of sharp metal waste | 9 (81.8) | 10 (100) | 5 (45.5) | 11(36.7) | 4 (50) | 39 (55.7) |
| Disposal of pathological/ anatomical waste | 9 (81.8) | 10 (100) | 4 (36.4) | 9 (30) | 0 | 32 (45.7) |
| Disposal of pharmaceutical waste | 5 (45.5) | 10 (100) | 1 (9.1) | 5 (16.7) | 0 | 21 (30) |
| Disposal of general waste | 9 (81.8) | 10 (100) | 10 (90.9) | 20 (66.7) | 4 (50) | 53 (75.7) |
| Treatment of BMW: preparation of disinfectant solution | 9 (81.8) | 10 (100) | 4 (36.4) | 8 (26.7) | 1 (12.5) | 32 (45.7) |
| Treatment of BMW: disinfection of plastic Materials | 7 (63.6) | 8 (80) | 0 | 6 (20) | 0 | 21 (30) |
| Final Disposal of BMW: sharp materials | 8 (72.7) | 6 (60) | 7 (63.6) | 13 (43.3) | 4(50) | 38 (54.3) |
| Final Disposal of BMW: anatomical waste | 7 (63.6) | 7 (70) | 1 (10) | 3 (10) | 1 (10) | 19 (27.1) |
Correct steps of BMWM are Segregation -Collection & Storage -Transport & Measurement -Treatment& Disposal. This is known to only one fourth of HCWs, but more than 60% could tell that segregation should be done at source. While enquired about disposal of waste, little higher than half (55%) could mention correctly disposal of sharp waste in white puncture proof container and 46% about disposal of anatomical or pathological waste in yellow bags. Regarding collection, storage and transport of the BMW, very few had correct knowledge. So far as treatment of BMW before disposal was concerned, less than half (46%) had idea about disinfection by bleaching solution and one third could tell that plastic materials would be disinfected or shredded or recycled before final disposal. Similarly 54% could tell the disposal of sharp materials in to sharp pit, but only 27% had idea about the disposal of anatomical waste in deep burial pit.
Attitude of the health care personnel towards BMWM
While assessing the attitude of the HCWs towards BMWM, more than 75% had positive attitude about the necessity of disinfection of hospital waste before disposal and 88% agreed about the necessity of BMW rule, but only 37% agreed that BMW management is essentially a team work. On the other hand, more than 50% HCWs completely agreed about the importance of segregation at source and about the fact that the improperly managed BMW might spread infection to the community. But while asked whether BMWM added an extra burden of work to them, 47% had positive attitude as they totally don't think it as burden, where as 41% agreed partially.
Practice of the health care personnel towards BMWM
The practice of the Health Care Workers was assessed by using an observation check list.
While assessing the disposal of BMW maintaining the colour code, only one fourth (25.7%) of the HCWs had correct practice. Regarding use of PPE (Personal Protective Equipment) during BMW handling, only one nurse was seen to have correct practice, that means she used all components of PPE. More than 70% had partially correct practice (those who used 2-3 essential components) and rest 27% had not used PPE (Table 3).
| Correct practice | Category of HCW | |||||
|---|---|---|---|---|---|---|
| Doctor (n=11) No (%) | N.S(n=10) No (%) | ph + lt (n=11) No (%) | h.s+anm (n=30) No (%) | Housekeeping staff (n=8) No (%) | Total (n=70) No(%) | |
| Disposal of BMW maintaining colour code | 7 (63.6) | 7 (70) | 2 (18.2) | 2 (6.7) | 0 | 18 (25.7) |
| PPE use at the time of BMW handling | 0 | 1 (10) | 0 | 0 | 0 | 1 (1.4) |
| Status of personal protection: vaccination | 0 | 0 | 0 | 0 | 0 | 0 |
| Status of personal protection: regular medical check up | 4 (36.4) | 1 (10) | 1 (9.1) | 2 (6.7) | 0 | 8 (11.4) |
| Status of training related to BMW | 8 (72.7) | 7 (70) | 1 (9.1) | 12 (40) | 3 (37.5) | 31 (44.3) |
As per the guidelines of BMWM, all HCWs should have completed vaccination of Hepatitis B and Tetanus Toxoid. It was observed that 47% had any one vaccine long time before and 53% had no vaccination at all. So far as regular medical check up was concerned, only 23% had irregular check up i.e at least one check up by medical practitioner in his/ her total service and 66% had never undergone any check up. More than 50% had no training on BMWM in last 1 year.
The study findings were evaluated across three domains (Knowledge, Attitude and Practice) for all the cadres of the study population. Six questionnaires in all the domains were selected for scoring with the opinion of three experts in public health.
It was revealed from Table 4 and Figure 1 that, knowledge and attitude score was seen better than practice score. The attitude score was very appreciable among the all categories of HCWs, whereas the knowledge score was highest among the nurses and very poor among the LTs & PHs and Housekeeping staff. In spite of good knowledge and attitude the practice was very poor among the all HCWs.
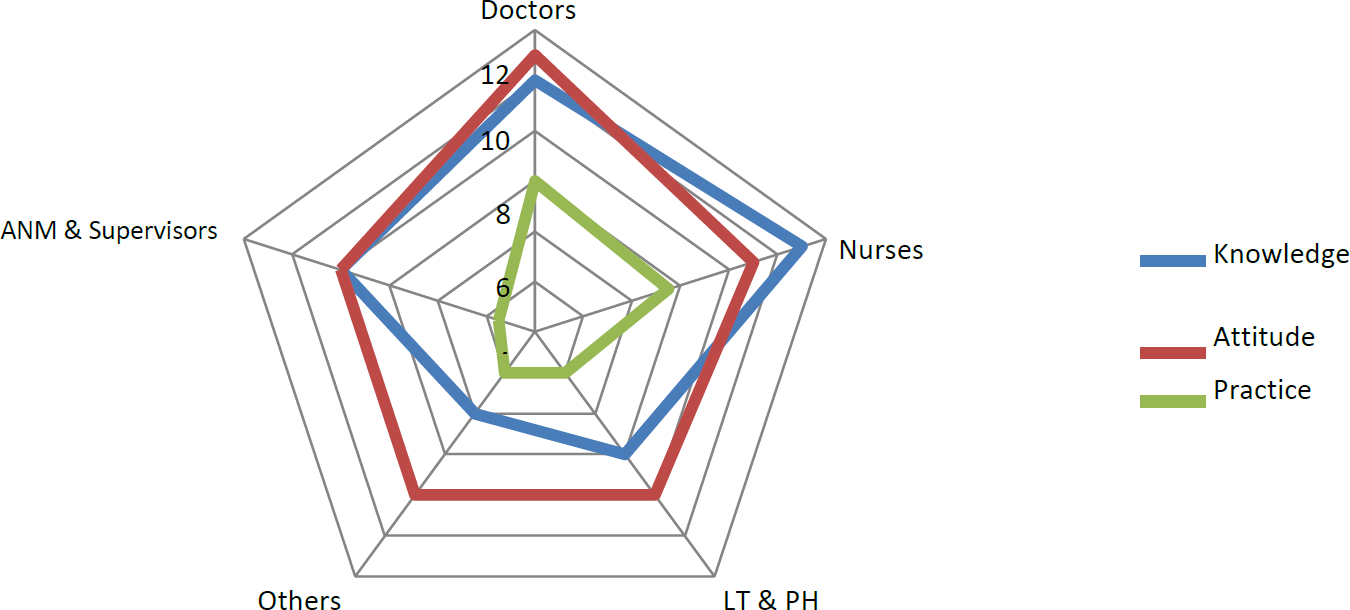
- DISTRIBUTION OF MEDIAN SCORE AMONG DIFFERENT CATEGORIES OF STUDY PARTICIPANTS
| Variable | Max Score | Range | Median | Q1-Q3 | Mean | SD |
|---|---|---|---|---|---|---|
| Knowledge Score | 12 | 0-12 | 8 | 5-10 | 7.5 | 2.84 |
| Attitude Score | 12 | 0-12 | 8 | 8-10 | 8.5 | 1.9 |
| Practice Score | 12 | 0-12 | 3 | 2-6 | 3.2 | 2.2 |
While finding association between the knowledge, attitude and practice score with age of the HCWs, those belong to the age group of < 30 years had the highest median knowledge and attitude score compared to 31-44 and in ≥ 45 years of age group, but the difference was not statistically significant. Similarly, the HCWs who had working experience for ≤10 years had the highest median knowledge score and those who were working for 11-19 years had the highest median score in attitude. But the practice score remained same among all of them. But in all cases the difference was not found statistically significant.
Gaps were found in selected primary health care facilities related to knowledge, attitude and practices of HCWs towards Bio-Medical Waste Management. Although nurses and doctors were knowledgeable, overall knowledge among other categories of the health care workers especially house keeping staffs was seen to be poor. Most of the HCW thought that BMW management added extra burden to them. Practice was seen to be poor inspite of having good knowledge and attitude. Training status, supervision and monitoring by higher officials were deficient.
DISCUSSION
Knowledge of the HCWS:
There were certain inadequacies in the different items of knowledge component among the HCWs in the present study. Less than two thirds of HCWs have correct knowledge about different categories of BMW and steps of BMW management, only 38.6% knew about hazards arising out of it. However, knowledge was comparatively better regarding colour coding (67%) and segregation at source (61.4%). In all respects nurses were most knowledgeable compared to doctors, HS & ANMs, paramedical workers and Housekeeping staff. In a study conducted in Sudan, HCWs had very good knowledge about categories of BMW and health hazards, but deficient in steps of management.9 Lavanya et al in Andhra Prodesh also found similarly, but knowledge was seen unsatisfactory in colour coding and principle of segregation.10 Choudasama et al in Rajkot however found better knowledge about health hazards, colour coding, steps of management, but deficient in identification of categories of BMW.11 Anand P et al in Haryana observed satisfactory knowledge about all the components among doctors than the nursing staff, lab technicians and sanitary staff.12 This difference might be due to different study setting, different categories of study population and due to difference in focus imparted on various components of BMWM during training.
Regarding disposal of different types of BMW, the present study found poor knowledge among the HCWs, except the general waste. In all aspects, housekeeping staff had very poor knowledge about all components of BMWM. Different studies conducted in India or abroad had similar findings.9-10,12-14 This finding is might be due to low educational level of these categories of staff, but is of high concern because they are mainly involved in transport and disposal of BMW. Again, nurses were found to have more correct knowledge in present study similar to Rao et al in Mysuru and Mondal R in Andhra Prodesh15. However, several studies17-18 found better knowledge among doctors due to better professional knowledge. Better knowledge among nurses can be explained by the discipline inherent in this nursing category of HCW, more involvement of them in applied work and task given by higher authority.
Attitude of the HCWS:
In the present study, the study participants showed positive attitude towards BMW management. Similar favourable attitude was shown in different studies. 9-10,13-14 But considering the BMWM as a team work, only 30% of the study participants agreed to it in present study. Contrary to that, almost 80% doctors and nurses in primary health care facilities in Lucknow, 90% of HCWs in a hospital of Sudan and 95% in Bihar considered it as team effort.9,14,19 In Lucknow 70% of the nurses and 90% of housekeeping staff thought BMWM as an extra burden to them.14 Similar to the present study (47%) around 40 to 50% of hCws in Sudan and Haryana of HCWs didn't consider it as burden.9,12 In the resource constrained primary health care facilities, the whole responsibility of BMWM is actually borne by the nursing and housekeeping staff, might be the possible reasons for their unfavourable attitude. Practice of the HCWS: Practice related to BMWM was seen to be very poor in the present study. Only one fourth of the HCWs were seen to dispose BMW maintaining colour code, practice was comparatively better among doctors and nurses. Contrary to that, in Sudan and Lucknow, more than 80% HCWs maintained disposal by colour codes.9,14 Use of PPE, status of vaccination and periodic medical check up were seen to be alarmingly poor in the present study, where as 75% and 62% of HCWs used PPE and took vaccination against Hepatitis B respectively in the study in Sudan.9 In Lucknow, vaccination was good among doctors, but not satisfactory among other staff.14 Similar was the picture of training in Lucknow14, where about 45% in the present study received training in last 1 year. A study in Rajkot also had similar finding.11
While scoring, the present study observed median score for domain of knowledge, attitude and practice being 8, 8, 3 respectively. Sekar M et al in a tertiary care hospital of Puducherrey found mean score as 6.04, 6.78 and 6.20 respectively.20 In Bangladesh the average score was found as 6.8± 1.2 varying from 7.3 (doctors) to 6.5 (internees).17 Knowledge was highest among nurses, followed by doctors, but very poor among paramedical and housekeeping staff in the present study. Ranu R et al however found doctors and Lab technicians as more knowledgeable than nurses and non medical staff in a tertiary setting in Trivandrum.18 So far practice was concerned, the present study observed very poor practice in all categories of HCWs in spite of having satisfactory knowledge and attitude. Sekar M in Puducherry found order of decreasing knowledge and practice among postgraduates followed by laboratory technicians, interns, nurses and sanitary staffs. Decreasing order of attitude was postgraduates, interns and laboratory technicians with same score, followed by nurses and sanitary staffs.20 However in few studies15,21,22 like the present one, nurses were seen to have better knowledge and practice compared to other categories. Reason might be due to more involvement of them in biomedical waste disposal.
Ranu R et al found significant increase in knowledge and practice level as the professional category level increases, but no relation with attitude.18 A statistically significant relationship was discovered between knowledge level and educational qualification, gender, work experience by Hossain F et al in Bangladesh.17 The present study found highest knowledge score in <=30 years age category and with the less years (<=10 years) of working experience than other groups, but no statistical significance was found. The difference might be difference of sample size as less number of study participants were available in primary health care facilities. The present study found gaps as in spite of having good knowledge and attitude, practice was seen to be poor. Similar finding was seen by Rao et al and Haque et al.15,19 Limitation of the study included less sample size of HCWs and lack of in depth interview of the staff to find out the reasons for poor knowledge and practice, which could not be contemplated due to pandemic situation.
CONCLUSION
Knowledge about the BMWM among the HCWs was mixed type. Knowledge among the Nurses was highest, followed by Doctors, ANMs & Health Supervisors, Pharmacists & Laboratory Technicians and lastly by the House keeping staff. Attitude of all HCWs was favorable regarding different aspects of BMWM, but many of them considered BMWM as an extra burden. In spite having good knowledge and attitude, practice was seen to be poor especially related to disposal following colour coding, segregation at source and use of PPE. None of them were properly vaccinated. Training status was also not satisfactory. There was no significant association with the median knowledge, attitude and practice score with age or years of experience of the study participants. For uplifting the knowledge and attitude of the HCWs repeated training and sensitization workshops should be organized. In micro level, practice of the health care workers should be monitored and supervised by ICN (Infection Control Nurse) and in macro level by block and district officials to evaluate the work and on the basis of that, next steps of planning should be formulated. To reduce health hazards, all the HCWs should be vaccinated properly with Hepatitis B vaccination and tetanus toxoid.
AUTHORS CONTRIBUTION
All authors have contributed equally.
REFERENCES
- Proper Management of Biomedical Waste Important to Curb COVID-19 Spread. Available at https://weather.com/en-IN/india/coronavirus/news/2020-10-21-management-biomedical-waste-important-curb-covid19-spread (accessed )
- [Google Scholar]
- Health Hazards of Medical Waste and its Disposal. Energy from Toxic Organic Waste for Heat and Power Generation. 2019:99-118. doi: 10.1016/B978-0-08-102528-4.00008-0. Epub 2018 Nov 9. PMCID: PMC7152398
- [CrossRef] [Google Scholar]
- In: Safe management of wastes from healthcare activities. (2nd). Geneva: World Health Organization; 2014. p. :11-12. Chapter 1,7
- [Google Scholar]
- Health-care waste. Available at https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed )
- [Google Scholar]
- Training manual on biomedical waste management for doctors, nurses, nodal officers and waste managers. Available at file:///E:/Documents/BMW%20paper/KAP%20article/D octors_manual_Added_Front_and_back_pg.pdf (accessed )
- [Google Scholar]
- Challenges to Healthcare in India -The Five A's. 2018. Indian J Community Med. 43:141-143. doi: 10.4103/ijcm.IJCM_194_18. PMID: 30294075; PMCID: PMC6166510
- [Google Scholar]
- Awareness about Biomedical Waste Management among Hospital Staff in a Tertiary Care Hospital in Tumkur. Indian Journal of Preventive Medicine. 2018;6(2) DOI: http://dx.doi.org/10.21088/ijpm.2321.5917.6218
- [Google Scholar]
- Knowledge, Attitudes and Practices regarding Biomedical Waste Management among staff of a tertiary healthcare centre in coastal Karnataka. J Pub Health Med Res. 2014;2(1):20-4.
- [Google Scholar]
- Assessment of Knowledge, Attitude and Practice of Biomedical Waste Management among Health Care Personnel at El-Mak Nimer University Hospital 2021. Journal of Health Statistics Reports SRC/JHSR-106. DOI: doi.org/10.47363/JHSR/2022(1)106
- [Google Scholar]
- M., Majhi P. Knowledge, Attitude and Practices (KAP) about biomedical waste management among hospital staff-A crossectional study in a tertiary care hospital, Andhra Pradesh, India. The Journal of Community Health Management, January-March. 2018;5(1):32-36.
- [CrossRef] [Google Scholar]
- Biomedical Waste Management: A study of knowledge, attitude and practice among health care personnel at tertiary care hospital in Rajkot. J Res Med Den Sci.. 2013;1:6-11.
- [Google Scholar]
- Knowledge, attitude and practice of biomedical waste management among health care personnel in a teaching institution in Haryana, India. Int J Res Med Sci. 2016;4:4246-50.
- [CrossRef] [Google Scholar]
- KAP study of bio-medical waste management among health care workers in Delhi. Int J Community Med Public Health. 2017;4:3332-7.
- [CrossRef] [Google Scholar]
- Knowledge, attitude and practices of biomedical waste management among health care personnel in selected primary health care centres in Lucknow. Int J Community Med Public Health. 2016;3:309-13.
- [CrossRef] [Google Scholar]
- Biomedical Waste Management: A Study on Assessment of Knowledge, Attitude and Practices Among Health Care Professionals in a Tertiary Care Teaching Hospital. Biomed Pharmacol J. 2018;11(3)
- [CrossRef] [Google Scholar]
- Knowledge, Attitude and Practice (KAP) Study Regarding Bio-Medical Waste Management Among Staff in a Tertiary Care Hospital at Andhra Pradesh. Asian Journal of Management. 2018;9(1):267-271. DOI: 10.5958/2321-5763.2018.00040.9
- [CrossRef] [Google Scholar]
- Factors associated with he current state of biomedical waste management knowledge, attitude, and practices among the healthcare professionals at a tertiary level hospital in Cumilla, Bangladesh. Natr Resour Human Health 2022:1-6. https://doi.org/10.53365/nrfhh/146613 eISSN: 2583-1194
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, Attitude and Practice Regarding Biomedical Waste Management amongst Health Care Personnel in a Medical College Hospital in Trivandrum. Ntl J Community Med. 2016;7(6):457-460.
- [Google Scholar]
- An Assessment of Knowledge, Attitude and Practices (KAP) of Bio-Medical Waste Management During Covid-19 Among Health Care Workers In A Tertiary Care Hospital of Bihar. 2021. International Journal of Health and Clinical Research,. 4:158-161.
- [Google Scholar]
- A study on knowledge, attitude and practice of biomedical waste management among health care workers in a Tertiary Care Hospital in Puducherry. Indian J Microbiol Res. 2018;5(1):57-60.
- [CrossRef] [Google Scholar]
- Knowledge, attitude, and practices about biomedical waste management as per 2016 rules among resident doctors and nursing staff in a tertiary care specialty hospital: A cross-sectional study. J Med Soc. 2020;34:31-5.
- [CrossRef] [Google Scholar]
- A study of knowledge attitude and practices of biomedical waste management at a tertiary care hospital, Kolkata. J Med Sci Clin Res. 2014;2:1930-40.
- [Google Scholar]




