
Translate this page into:
A Study on Knowledge and Attitude on Comprehensive Abortion Care (CAC) among Married Women of Reproductive Age Group with a View to Develop an Awareness Program in a Selected Rural Community, West Bengal
Corresponding author: Prof(Dr.)Mausumi Basu, MD, FAIMER Fellow, MAMS, Department of Community Medicine, IPGME&R and SSKM Hospital, Kolkata, India, Mobile no: +91 9231441362 Email: basu.mausumi544@gmail.com
How to cite this article: Roy B, Choudhuri M, Dutta S, Mandal MM, Saha SK, Mausumi Basu M. A Study on Knowledge and Attitude on Comprehensive Abortion Care (CAC) among Married Women of Reproductive Age Group with a View to Develop an Awareness Program in a Selected Rural Community, West Bengal. J Comprehensive Health 2020;8(2): 49-54.
Abstract
Introduction:
Comprehensive Abortion Care (CAC) implies that women must be able to access high-quality, affordable abortion care in the communities where they live and work.
Objectives:
To assess the knowledge and attitude regarding CAC among married women of reproductive age group in selected rural community, West Bengal India.
Materials and Methods:
A descriptive type of observational study, cross sectional in design was conducted among 400 married women of reproductive age group in selected villages of Gazole and Bamongla Block of Malda District using a pre designed pre tested structured schedule from 9/2017 to 9/2018, a period of 1 year. Data were tabulated in Microsoft Office Excel 2010 and analysis was done using Statistical Package for the Social Sciences (SPSS) Version 20.0.
Results:
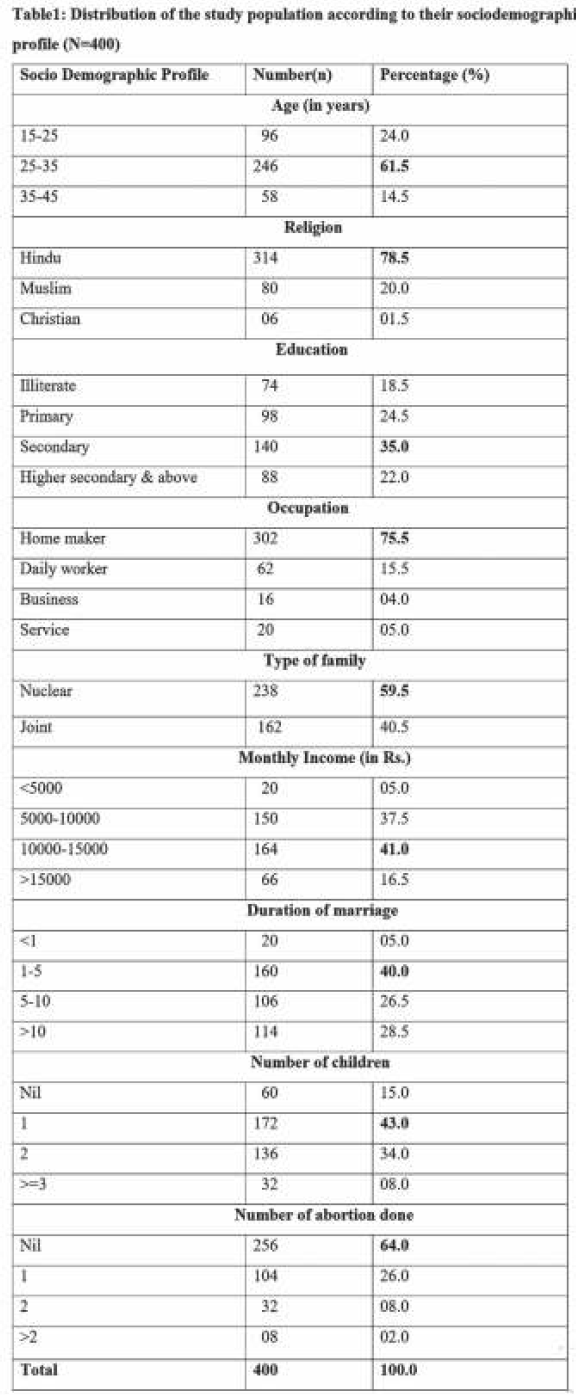
About 61.5% belonged to age group of 25-35 years, 78.5% followed Hinduism, 35% completed Secondary education, 59.5% came from nuclear family, 75.5% were home makers, 43% had one child, 64% not opted for abortion, 66% had adequate knowledge, 78% had positive attitude, 55.5% knew meaning of abortion, 78.5% knew place for termination of pregnancy, 76.5% told best method to prevent unwanted pregnancy, 87.5% told why Comprehensive Abortion Care is important.
Conclusion:
Awareness programme on Comprehensive Abortion Care through mass media and interpersonal communication should be initiated at programmatic level.
Keywords
Comprehensive Abortion Care
Knowledge
Attitude
Reproductive age group

Introduction:
Government of India (GOI) launched the Reproductive and Child Health Program (RCH) since October 1997. Among the different strategies of reproductive health, safe/legalized abortion in India has remained neglected so far.[1] Unsafe/illegal abortion is a significant but preventable cause of maternal mortality.[2] Lack of available, accessible, effective, safe abortion services by qualified persons in hygienic condition and absence of knowledge regarding the same in the community is one of the important reasons even after more than 45 years of enactment of MTP 1971 act In India.[3] Fortunately, this aspect is being reviewed now.
Comprehensive Abortion Care (CAC),[4] under the Ministry of Health & Family Welfare, National Health Mission (NHM) is a term "rooted in the belief that women must be able to access high-quality, affordable abortion care in the communities where they live and work", was first introduced in India by Ipas in 2000.[5] After successful pilot studies in three states, transformation of abortion services from only clinical procedures to a comprehensive women-centred service from conception up to post abortion care including pain management were gained impetus. One of the important successes of those efforts was changing the terminology from MTP to CAC, thus accepting the centrality of the woman.[5] Comprehensive Abortion Care includes all of the elements of post abortion care (PAC)[Treatment, Counselling, Contraceptive & Family Planning, Reproductive & other health services] as well as safe abortion care (SAC).[6] In 2015-19, there were on average 1210 million unintended pregnancies each year globally, equal to a global annual rate of 64 unintended pregnancies/1000 women aged 15-49 years means 48% were unintended. In the same time, there were 73•3 million abortions annually, corresponding to a global annual rate of 39 abortions / 1000 women aged 15-49 years means that 61% of unintended pregnancies had abortion.[7]
As per WHO Lancet study, out of the total 48.1 million pregnancies in India, estimated unintended pregnancy rate was 70/ 1,000 women aged between 15-49 in 2015.[8]
A study conducted by the International Institute for Population Science (IIPS), Mumbai, the Population Council, New Delhi and the Guttmacher Institute based in New York found that an estimated 15.6 million abortions occurred in 2015 in India and the abortion rate was 47/1000 women aged 15-49 years. About 81% used medication abortion method (MMA), 14% carried out surgical abortion method, and the rest 5% abortions were carried out outside the health facilities using other (probably unsafe) methods. Around 22% of abortions in India took place in health facilities, 73% used drugs from chemists and informal vendors, outside the health facilities (MMA) and 5% did outside of health facilities using methods other than medication abortion.[9]
With this background a study was conducted with the objective of assessing the knowledge and attitude regarding CAC among married women of reproductive age group in selected rural community, West Bengal India.
Materials and Methods:
A descriptive type of observational study, cross sectional in design was conducted among married women of reproductive age group in selected villages of Gazole and Bamongla Block of Malda District, West Bengal, India from 9/2017 to 9/2018, over a period of 1 year. Inclusion criteria were 15-45 years married women, permanent resident of the village, present during the data collection period and gave informed written consent to participate in the study Seriously ill women were excluded from the study. Study tool was a pre designed pre tested structured schedule, Likert scale, structured opinionnaire. The schedule had four partsPart I Consisted of information on the socio-demographic profile; Part II consisted of questions on knowledge about comprehensive abortion care; Part III dealt with questions regarding attitude about comprehensive abortion care and Part IV was Opinionnaire for evaluation of the awareness program The schedule was designed in consultation with three experts; 2 from nursing field and 1 from gynaecology & obstetric depart-ment, it was pretested on 20 married women of reproductive age group of the same blocks; then modified, necessary changes were done and validated by another 3 experts. Study technique was face-to-face interview and all questions were asked in local languages.
Study variables were:
A. Socio-demographic profile (age, religion, education occupation, type of family, number of family members, PCMI, duration of marriage, parity, H/O abortion), B. 18 knowledge questions (1. Meaning of abortion, 2. ideal place of pregnancy termination, 3. maximum period for undergoing abortion is safe, 4. best method to prevent unwanted pregnancy, 5. physical condition during pregnancy a women need to terminate the pregnancy, 6. factors leads a woman to undergo abortion, 7. where a woman gets service for comprehensive abortion care, 8. importance of Comprehensive Abortion Care, 9. Abortion counseling involves what, 10. Causes of illegal abortion, 11. which is not a reproductive right, 12. beneficiaries of CAC, 13. follow up after abortion, 14. best method to maintain spacing, 15. When a woman should start using contraception after abortion, 16. CAC service considers the need of the woman, 17. factors act as barrier for CAC service, 18. NOT mandatory for abortion procedure), C. 24 attitude questions (Some are mentioned here as an example like 1. Unsafe abortion is a serious health problem, 2. Repeated abortion is dangerous for women health, 3. Woman who have an abortion are ending a life, 4. Woman prefers to have medical abortion rather than surgical abortion, 5. Abortion service should be available to every woman, who wants this service, 6. The barriers of comprehensive abortion services are lack of awareness, 7. Use contraceptive is much more desirable than having abortion, 8. A woman should be able to have an abortion even if her husband wants her to continue the pregnancy), D. 8 questions of opinionnaire to determine opinion of acceptability of the awareness programme (1. The awareness programme is helpful for learning, 2. The programme gives information which is necessary about Comprehensive Abortion Care, 3. The programme gives adequate knowledge about Comprehensive Abortion Care., 4. The content covered the different area of Comprehensive Abortion Care, 5. The language used in the programme is simple and clear, 6. The A.V. aids used in the programme are well illustrated, 7. The overall appearance of the programme is attractive, 8. The organization of the programme is systematic).
Sample size was calculated using the formula, N = Z2pq/L2, where N= initial sample size, Z=1.96, p=proportion of study population with adequate knowledge, q=1-p, L=Allowable error (10% of p). Assuming 50% had adequate knowledge, with a absolute precision of 5% and 95% level of confidence, the sample size was calculated as 384. After adding non response rate of 5%; the final sample size was 403(roughly 400).
Multistage Sampling technique was followed: Stage 1: From15 Blocks of Malda District (9 Blocks in Malda Sadar Subdivision plus 6 Blocks in Chanchal Subdivision), 15% (2) blocks were selected by simple random sampling method. These two blocks were
a. Gazole and
b. Bamongla.
Stage 2:
From those 2 Blocks, three (3) and one(1) villages were selected respectively by simple random sampling technique(proportionately with number of villages, as the total number of villages of Gazole and Bamongola Blocks are 286 and 141 respectively).
Stage 3:
Hundred (100) population from each village were selected by simple random sampling technique.
This study was conducted after taking permission from Ethics Committee of IPGME & R, SSKM Hospital, Kolkata.
Data were tabulated in Microsoft Office Excel 2010 (Microsoft Corp, Redmond, WA, USA) and analysis was done using Statistical Package for the Social Sciences (SPSS) Version 20.0.
Operational definition:
Comprehensive Abortion Care- Comprehensive Abortion Care strives to provide safe, high-quality services, including abortion, post abortion care and family planning. [National Health Mission. Comprehensive Abortion Care-CAC.[4]
Reproductive age group-
Women of reproductive age refers to all women aged 15-49 years.
Illiterate -
A person can be considered illiterate if he/she cannot read and write with understanding in any language should be above 7 years of age.
Knowledge score calculation-
Knowledge was assessed on 18 questions. Each correct response was scored one (1) while incorrect/don't know zero (0). Adequate knowledge was score >11 (Median score).
Attitude score calculation-
For 24 items, 5 point Likert Scale was used, from Strongly disagree, Disagree, Undecided, Agree, Strongly agree, given a score of one(1),two (2), three(3), four(4) and five(5) respectively. Those having median score S84 were said to have positive attitude.
Results:
Socio-demographic profile of the study population were demonstrated in Table 1. Out of total 400 study population who were interviewed, majority (61.5%) belonged to the age group of 25-35 years with mean age of 30.7± 8.3 years and about 78.5% followed Hinduism. Regarding education, about 35% completed Secondary education whereas 18.5% were illiterate. About 59.5% came from nuclear family, 75.5% were home makers, 41% were married for 1 to 5 years, 43% had one child, and 64% not opted for abortion. About 41% of the study population had monthly family income of Rs. 10000- 15000.
Data presented in Table 2 revealed that the knowledge score of married women of reproductive age group ranged between 3-18 with a mean score of 11.52, median 11, standard deviation 2.79, and Interquartile range was 4. Similarly the attitude score ranged between 24-120 with a mean score of 84.45, median 84, standard deviation 8.31, and Interquartile range was[10].

Indicators of knowledge of the study population were showed in Table 3. About 55.5% knew correctly the meaning of abortion, 78.5% told correctly the place for termination of pregnanc, 76.5% knew the best method to prevent unwanted pregnancy, and 87.5% told correctly why Comprehensive Abortion Care is important. Factor that leads a woman to undergo abortion was known by 88.5%, cause of illegal abortion in our country was told by 82%, and best method to maintain spacing between two child births was known by 83%. Family members opinion is not mandatory for abortion procedure was known by 64.5%, and lack of awareness is the main barrier for CAC service was told by 67% of the study population. The less known part of information consisted mainly of maximum period for undergoing safe abortion for a woman (26.5%), follow-up after abortion (37%), who are the beneficiaries for CAC(50%),when a woman should start using contraception after abortion(53%) and which is not a reproductive right (47%).

Data presented in component bar diagram revealed that 264(66%) of the study population had adequate knowledge whereas 312(78%) woman of reproductive age group had positive attitude regarding CAC (Figure 1).
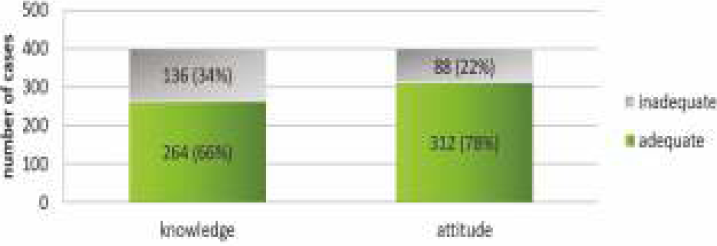
- Distribution of the study population according to Knowledge and Attitude regarding Comprehensive Abortion Care (N=400)
Correlation co-efficient and their significance between knowledge score of the Woman of reproductive age group and their attitude towards CAC described that 'r' value computed between knowledge and attitude score was 0.074, indicating very weak correlation between the two variables. The calculated 't' value between knowledge and attitude was 1.04, which is not statistically significant at 0.05 level of significance (Figure 2).
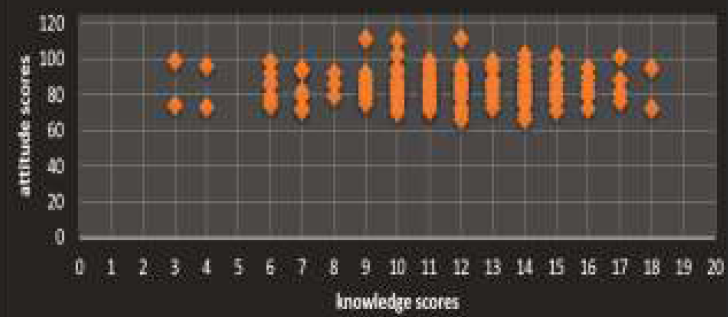
- Scatter plot of knowledge versus attitude
Acceptability of the awareness program-Almost all of the study population (99%) were strongly agreed that the awareness program regarding CAC were helpful for learning, it also provided necessary information about Comprehensive abortion care.
Discussion:
Unsafe/illegal abortions account for 8% of all maternal deaths in India. The barriers which impede women from reaching the required safe abortion services include illiteracy especially female illiteracy, lack of awareness, lack of access to health facilities, distance, lack of confidentiality, anonymity, privacy and respect towards women.
This study has tried to assess knowledge and attitude on Comprehensive Abortion Care (CAC) among married women of reproductive age group in selected rural community of West Bengal, India.
The present study finding indicates that majority (61.5%) of the study population belonged to the age group of 25-35 years with mean age was 30.7±8.3 years which was more than a study conducted by Adera et al at Ethiopia 9 among Women of Reproductive age group (37.8%), Bamnia et al at Mewar, Rajasthan 10 (56%), Cresswell et al at Zambia (33%) 11, Banerjee et al at Bihar and Jharkhand (56%)12, Srivastava et al at Indore(53.33%)13 and Khanal et al at Nepal(47%).14In the present study 40.5% participants belonged to joint family whereas it was 56% at Bihar and Jharkhand.12 In our study 19% were illiterate which was almost similar to Ethiopia (16%)8, but lower than Rajasthan (40%)10 & Indore (40.5%) 13 and higher than Zambia(4%). 11 About 43% women had one child in this study, which was nearly similar to Rajasthan (33%)10 and Indore (33.8%). 13 This study revealed that 64% had no abortion history, whereas in Bihar and Jharkhand 85.7% had no spontaneous abortion and 95.4% had no induced abortion. 12 About 14% of women reported at least one spontaneous abortion, while induced abortions were reported by only 5% of women in Bihar and Jharkhand12, which was much less than our study (26%).
Regarding knowledge, 76% knew correctly about conditions in which a pregnant mother can have a legal abortion service in Ethiopia 9 which was in line with this study (71%). On the contrary, just 16% of women of reproductive age correctly identified the grounds for which abortion is legal in Zambia.11 Only 40% of women of reproductive age group knew that the extreme situation where the pregnancy threatens the life of the mother was grounds for a legal abortion. About 55% of study population answered the definition of abortion correctly in the present study while 38% defined correctly in Ethiopia 9 and 23.8% in Nepal.14 Among the sampled population only 26.5% knew about the time for eligible termination of pregnancy, in contrast to 77% of Ethiopia 9 and 70% in Nepal.[14] About 78.5% of the respondents knew safe abortions are performed at government approved institutions which was similar to Nepal (68.9%)14 but higher than Mewar (58%)10 and Bihar (46%).12 About 27% of participants were aware about the usage of contraceptives in Mewar 10 in contrast to 53% in the present study. The main reason for undergoing abortion was failed contraception followed by unplanned pregnancies in Mewar 10 and Indore (38.1% and 32.38%) [13] in contrast to this study where it was unplanned pregnancy (88%). We found that gestation limits for legal MTP was known by 26.5% which was much higher than Bihar 12 where it was only 1.9%. Though the MTP Act has existed for almost five decades in India, more than half of the women in this study and Bihar study were unaware that abortion is legal in India, and very few of them were aware of particular aspects of the law.12On the whole, the level of satisfactory knowledge of abortion among the women interviewed was 66% and in Nepal it was 53.5%.[14]
Women's attitudes towards abortion were not very conservative unlike Zambia study.11Only 22% of the participants of this study had not positive attitude towards abortion, similar to Ethiopia study (23%).9In Zambia 11 majority of the women (90%) had poor attitude regarding Comprehensive Abortion Care. More than 90% of women either agreed or strongly agreed with the statement 'abortion is immoral' in Zambia study[11], in line with our study (82%). Conversely, the majority of women either disagreed or strongly disagreed with the statements 'women should have access to safe abortion services' (86%); like Zambia study (81%) 11and 'unmarried women should have access to safe abortion services' (79%).
Limitations:
Like other studies, our study also has some limitations. Self-reported information may be subjected to reporting errors, missed values &social desirability bias. Cross- sectional study design was used in the present study. Measuring attitudes quantitatively is complex. The findings of this study are based on only two blocks of one selected district and cannot be generalized to the whole of West Bengal.
Strength-
The study was a population-representative, community-based survey with a good sample size. We were able to collect data on a large number of variables relating to CAC.
Conclusion:
Our findings showed satisfactory knowledge and positive attitude of the married women of reproductive age group regarding Comprehensive Abortion Care were 66% and 78% respectively. We need to impart awareness programme on Comprehensive Abortion Care. The concept of CAC was well accepted to the married women of reproductive age group and they are interested to learn more regarding CAC. However, changing community knowledge and attitudes is challenging, especially when the topic is stigmatised. Additional interventions are needed like spreading of awareness through mass media and interpersonal communication.
References:
- RMNCH+A. Maternal Health. State Health Society. National Health mission. Health and Family Welfare Department. Available from https://nhm.gujarat.gov.in/comprehensive-abortion-care.htm (accessed )
- [Google Scholar]
- Unsafe abortion: the preventable pandemic. The Lancet. 2006;368(9550):1908-19.
- [CrossRef] [PubMed] [Google Scholar]
- The Medical Termination Of Pregnancy Act, 1971. Department Of Health & Family Welfare. Ministry of Health and Family Welfare. GOI. Available from https://main.mohfw.gov.in/acts-rules-and-standards- health-sector/acts/mtp-act-1971 (accessed )
- [Google Scholar]
- Department of Health & Family Welfare. National Health Mission. GOI. Available from https://hfw.assam.gov.in/ schemes/comprehensive-abortion-care-0 (accessed )
- [Google Scholar]
- Comprehensive Abortion Care. Available from https://www. ipasdevelopmentfoundation.org/comprehensive-abortion-care.htm (accessed )
- [Google Scholar]
- A service of the National Library of Medicine, National Institutes of Health. Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings: 2010 Revision for Field Review. Geneva: Inter-agency Working Group on Reproductive Health in Crises; 2010. Available from https://www.ncbi.nlm. nih.gov/books/NBK305158/?report=printable (accessed )
- [Google Scholar]
- Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990-2019. Lancet Glob Health 2020 Published online July 22, 2020 https://doi.org/10.1016/S2214-109X(20)30315-6. Available from https://www.thelancet.com/journals/langlo/home (accessed )
- [CrossRef] [PubMed] [Google Scholar]
- The Incidence of abortion and unintended pregnancy in India, 2015. Lancet Glob Health. 2018;6(1):e111-e120.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of Knowledge, Attitude and Practice Women of Reproductive Age Group towards Abortion Care at Debre Markos Referral Hospital, Debre Markos Ethiopia. Science Journal of Public Health. 2015;3(5):618-624.
- [CrossRef] [Google Scholar]
- The study of knowledge, attitude and practice about abortion and technology at the tertiary centre in the region of Mewar, Rajasthan, India. Int J Reprod Contracept Obstet Gynecol. 2018;7(8):3320-4.
- [CrossRef] [Google Scholar]
- Women's knowledge and attitudes surrounding abortion in Zambia: a cross sectional survey across three provinces. BMJ Open. 2016;6:e010076. doi:10.1136/bmjopen-2015-010076.
- [CrossRef] [PubMed] [Google Scholar]
- Woman- centered research on access to safe abortion services and implications for behavioral change communication interventions: a cross-sectional study of women in Bihar and Jharkhand, India. BMC Public Health. 2012;12:175.
- [CrossRef] [PubMed] [Google Scholar]
- The study of knowledge, attitude and practice of medical abortion in women at a tertiary centre. IOSR Journal of Dental and Medical Sciences. 2015;14(12):2279-0861.
- [Google Scholar]
- Knowledge and Practice of Abortion among Women in Nepal. Asia-Pacific E-Journal of Health Social Science. 2014;3(1):1-6.
- [Google Scholar]




